The issue of uninsured Americans remains a pressing concern in the United States, with millions of individuals lacking access to adequate healthcare coverage. Despite efforts to expand insurance options through initiatives like the Affordable Care Act, a significant portion of the population continues to face barriers to obtaining health insurance. Factors such as high premiums, limited employer-sponsored plans, and gaps in public programs contribute to this persistent problem. Understanding the scope and implications of this issue is crucial, as it not only affects individual health outcomes but also places a substantial burden on the broader healthcare system and economy.
Explore related products






What You'll Learn
![]()
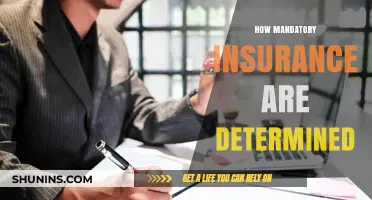
Uninsured rates by state
Texas leads the nation in uninsured rates, with approximately 18% of its residents lacking health coverage as of 2023. This figure is nearly double the national average of 9.1%, highlighting a stark disparity in access to healthcare. The state’s high uninsured rate is partly attributed to its decision not to expand Medicaid under the Affordable Care Act, leaving many low-income adults in the "coverage gap"—earning too much to qualify for traditional Medicaid but too little to afford private insurance. Additionally, Texas has a large population of undocumented immigrants, who are ineligible for federal health programs, further inflating the uninsured numbers.
In contrast, states like Massachusetts and Vermont boast the lowest uninsured rates, hovering around 3% and 4%, respectively. Massachusetts’ success is often tied to its early adoption of a state-level health insurance mandate in 2006, which served as a model for the ACA. Vermont’s low rate can be attributed to its robust Medicaid expansion and state-funded programs that target vulnerable populations, including children and low-income families. These states demonstrate that policy decisions at the state level can dramatically reduce uninsured rates, even in the absence of federal uniformity.
Southern states consistently rank among the highest in uninsured rates, with Mississippi, Georgia, and Florida trailing closely behind Texas. Common factors include resistance to Medicaid expansion, lower median incomes, and a higher proportion of workers in industries that do not offer employer-sponsored insurance, such as agriculture and service sectors. For example, in Mississippi, nearly 13% of residents fall into the coverage gap, and the state’s uninsured rate stands at 13.8%. This regional trend underscores the intersection of economic and policy barriers in the South.
To address these disparities, states with high uninsured rates could consider targeted interventions. Expanding Medicaid is the most direct solution, as seen in states like Oklahoma and Missouri, where voter-approved expansions led to immediate reductions in uninsured rates. Additionally, increasing funding for community health centers and implementing state-level subsidies for private insurance could bridge gaps in coverage. For individuals in high-uninsured states, practical steps include exploring ACA marketplace plans during open enrollment, checking eligibility for Medicaid or CHIP (Children’s Health Insurance Program), and utilizing free or low-cost clinics for immediate healthcare needs.
While federal policies provide a framework, the variation in uninsured rates by state reveals the critical role of local decision-making. States with proactive measures, like Medicaid expansion and state-funded programs, have successfully lowered uninsured rates, while others lag due to policy inertia or economic challenges. Understanding these state-level differences is essential for both policymakers and individuals navigating the complexities of healthcare access in the U.S.
Life Insurance Agent Exam: How Many Questions to Expect?
You may want to see also
Explore related products






![]()
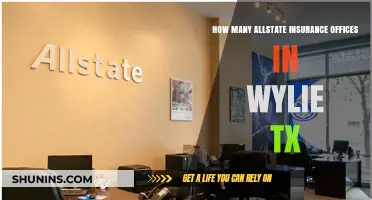
Impact of income on coverage
Income is a critical determinant of health insurance coverage in the United States, with a stark divide between higher and lower earners. According to the U.S. Census Bureau, in 2022, 8.5% of Americans were uninsured, but this rate varies dramatically by income level. Among individuals living below the federal poverty level (FPL), the uninsured rate was 18.3%, compared to just 4.5% for those with incomes at or above 400% of the FPL. This disparity highlights how financial constraints directly limit access to healthcare, as lower-income individuals often cannot afford premiums, deductibles, or out-of-pocket costs, even with subsidized options available through the Affordable Care Act (ACA).
To bridge this gap, understanding the mechanics of income-based subsidies is essential. For instance, ACA marketplace plans offer premium tax credits to individuals earning between 100% and 400% of the FPL. A single person earning $13,590 to $54,360 annually in 2023 qualifies for these credits, which can reduce monthly premiums significantly. However, those below 100% of the FPL often fall into the "coverage gap" in states that did not expand Medicaid, leaving them without affordable options. Conversely, employer-sponsored insurance (ESI) is more common among higher earners, with 72% of workers in the top income quartile having access, compared to 44% in the bottom quartile. This disparity underscores the role of income in shaping coverage pathways.
A comparative analysis reveals that income not only affects the *type* of coverage but also its *quality*. Lower-income individuals are more likely to enroll in plans with higher deductibles and narrower networks, limiting their access to care. For example, a Silver-level ACA plan might have a deductible of $4,000 for someone earning 200% of the FPL, whereas a higher earner might opt for a Gold plan with a $1,000 deductible. This trade-off between affordability and comprehensiveness disproportionately impacts those with limited financial resources, perpetuating health disparities.
Practically, addressing the income-coverage gap requires targeted interventions. Expanding Medicaid in non-expansion states would cover an estimated 2.2 million uninsured adults in the coverage gap. Additionally, capping marketplace premiums at 8.5% of income, as implemented by the American Rescue Plan, has already reduced costs for millions. For individuals, leveraging tools like Healthcare.gov’s subsidy calculator can help determine eligibility for financial assistance. Employers can also play a role by offering more affordable ESI options to low-wage workers, though this remains less common in industries like retail and hospitality.
In conclusion, income’s impact on health insurance coverage is both profound and multifaceted, shaping not only who is insured but also the quality of coverage obtained. Policymakers, employers, and individuals must work collaboratively to dismantle financial barriers, ensuring that access to healthcare is not a privilege reserved for the affluent but a right accessible to all, regardless of income.
Cancer and Term Life Insurance: Does Level Death Benefit?
You may want to see also
Explore related products
![[*Mini Size*] TIRTIR Mask Fit Red Cushion Foundation | Full coverage, Weightless, Skin fit, Satin Glow Finish, Korean Makeup, beauty, Tattoo cover up, Buildable (#22N Shell Beige, 0.15 Fl Oz)](https://m.media-amazon.com/images/I/71qYxmRW4aL._AC_UY218_.jpg)





![]()
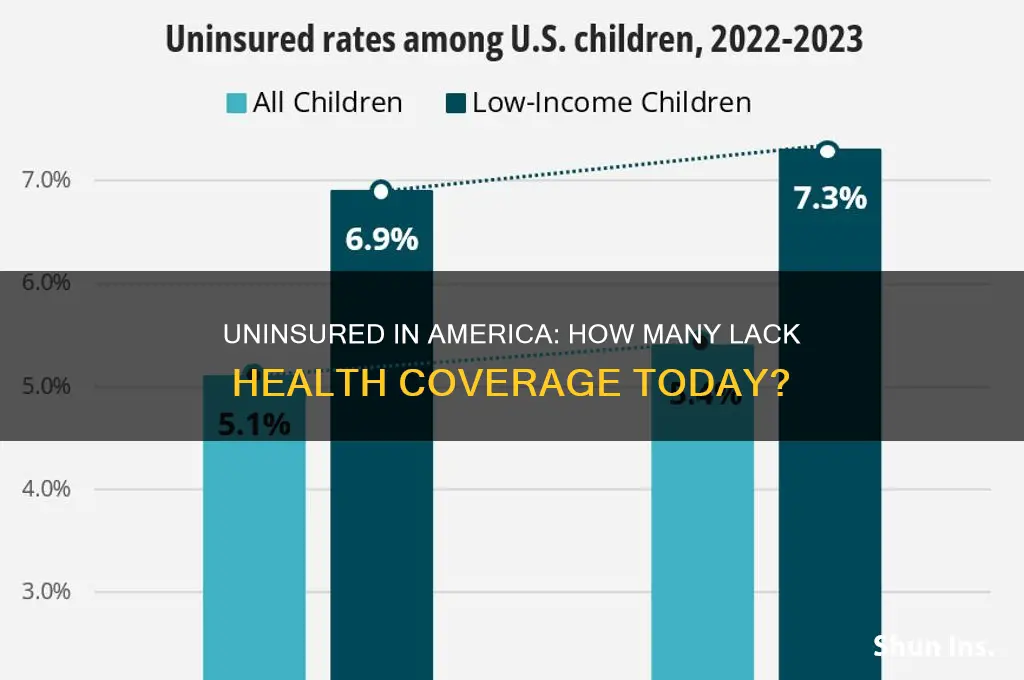
Racial disparities in insurance
According to recent data, approximately 8.5% of Americans, or about 28 million people, were uninsured in 2022. However, this figure masks significant racial disparities in insurance coverage. For instance, while 5.4% of non-Hispanic whites lack insurance, the rate jumps to 9.6% for African Americans and 18.3% for Hispanics. These disparities are not merely numbers but reflect systemic inequalities that affect health outcomes, financial stability, and overall well-being.
Analyzing the Root Causes
Practical Steps to Address Disparities
To mitigate these disparities, policymakers and advocates can take targeted actions. Expanding Medicaid in the 10 states that have not yet done so would immediately reduce uninsured rates among minorities, as these states have disproportionately high Black and Hispanic populations. Employers can also play a role by offering affordable health plans to low-wage workers, regardless of full-time status. Community-based initiatives, such as enrollment fairs and multilingual outreach, can help bridge the gap in awareness and access to insurance options like the Affordable Care Act (ACA) marketplace.
Comparative Perspective: Lessons from Successful Models
States like California and New York have made strides in reducing racial disparities in insurance coverage by implementing aggressive outreach programs and expanding Medicaid eligibility. California, for instance, covers undocumented young adults up to age 26 under its Medicaid program, significantly benefiting its large Hispanic population. In contrast, states with higher uninsured rates among minorities often lack such inclusive policies. By studying these models, other states can adopt strategies that prioritize equity and inclusivity in healthcare access.
The Human Cost and Long-Term Implications
The consequences of racial disparities in insurance extend beyond financial strain. Uninsured individuals are less likely to receive preventive care, leading to higher rates of chronic conditions like diabetes and hypertension, which disproportionately affect communities of color. For example, African Americans are 60% more likely to have diabetes than non-Hispanic whites, yet they are less likely to have insurance to manage the condition. This cycle of poor health and limited access perpetuates economic inequality, as untreated illnesses often lead to lost wages and reduced productivity. Addressing these disparities is not just a moral imperative but an economic necessity.
Does Root Insurance Offer a Grace Period? What You Need to Know
You may want to see also
Explore related products



![]()
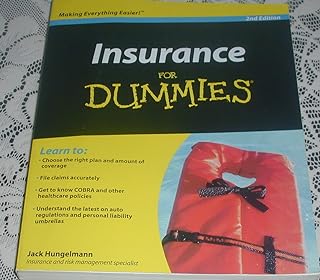
Uninsured children statistics
As of recent data, approximately 4.3 million children in the United States lack health insurance, a figure that underscores a persistent gap in coverage despite broader national efforts to expand access. This statistic is particularly alarming when considering the developmental and health needs of children, who require consistent access to preventive care, immunizations, and treatment for illnesses or injuries. The uninsured rate for children, though lower than that of adults, remains a critical issue due to the long-term consequences of inadequate healthcare during formative years.
Analyzing the demographics reveals disparities that demand attention. Children in low-income families are disproportionately affected, with Medicaid and the Children’s Health Insurance Program (CHIP) serving as primary safety nets. However, administrative barriers, such as complex enrollment processes or lapses in coverage due to periodic eligibility checks, leave some children vulnerable. Additionally, geographic variations play a role; states that have not expanded Medicaid under the Affordable Care Act often report higher rates of uninsured children, highlighting the impact of policy decisions on access.
From a practical standpoint, addressing this issue requires targeted interventions. Schools and community health centers can serve as vital access points for uninsured children, offering screenings, vaccinations, and referrals to affordable care options. Parents and caregivers should be educated about available programs like CHIP, which provides low-cost coverage for children in families who earn too much to qualify for Medicaid but cannot afford private insurance. Simplifying enrollment processes and ensuring continuous coverage through automatic renewals could significantly reduce the number of uninsured children.
A comparative perspective reveals that while the U.S. has made strides in reducing child uninsured rates over the past two decades, it lags behind peer nations with universal healthcare systems. For instance, countries like Canada and the UK report near-zero rates of uninsured children, emphasizing the role of systemic solutions in achieving comprehensive coverage. This comparison underscores the need for policy reforms that prioritize universal access for children, regardless of family income or state of residence.
Ultimately, the persistence of uninsured children in the U.S. is not just a statistical concern but a moral and economic imperative. Uninsured children are more likely to face delayed treatment, poorer health outcomes, and higher healthcare costs in the long run. By focusing on policy reforms, community-based solutions, and streamlined access to existing programs, the nation can move closer to ensuring that every child has the healthcare they need to thrive.
Is Schwab SIPC Insured? Understanding Your Investment Protection
You may want to see also
Explore related products




![]()
Effect of policy changes on rates
Policy changes have a direct and measurable impact on the number of uninsured Americans, often shifting rates in predictable ways depending on the nature of the reform. For instance, the Affordable Care Act (ACA) of 2010 expanded Medicaid eligibility and established health insurance marketplaces, leading to a significant drop in the uninsured rate from 16% in 2010 to 8.6% in 2016. This example illustrates how comprehensive policy interventions can reduce barriers to coverage, particularly for low-income individuals and families. Conversely, attempts to repeal or weaken such policies, like the 2017 effort to dismantle the ACA, have threatened to reverse these gains, highlighting the fragility of progress in this area.
Analyzing the mechanics of these changes reveals that policy effectiveness hinges on accessibility and affordability. For example, the ACA’s subsidies for marketplace plans made coverage attainable for millions of middle-income Americans, while Medicaid expansion addressed gaps for those earning up to 138% of the federal poverty level. However, states that opted out of Medicaid expansion saw persistently higher uninsured rates, demonstrating the critical role of state-level adoption in federal policy success. This underscores the importance of aligning federal initiatives with state participation to maximize impact.
A comparative look at policy changes pre- and post-ACA further clarifies their effects. Before the ACA, employer-based insurance was the primary coverage source, leaving gaps for part-time workers, self-employed individuals, and those in low-wage jobs without benefits. The ACA’s individual mandate and guaranteed issue provisions filled these gaps, though the mandate’s repeal in 2019 contributed to a slight uptick in uninsured rates. This comparison suggests that policies must address both systemic gaps and individual barriers to maintain progress.
Practical takeaways for policymakers and advocates include prioritizing policies that simplify enrollment processes and reduce out-of-pocket costs. Auto-enrollment strategies, for instance, have shown promise in states like California, where they increased Medicaid participation by streamlining sign-ups. Additionally, capping marketplace premiums at 8.5% of income, as implemented in the American Rescue Plan Act of 2021, made plans more affordable for millions. Such targeted measures can mitigate the effects of broader economic factors, like inflation or job loss, that might otherwise drive up uninsured rates.
Ultimately, the effect of policy changes on uninsured rates is a dynamic interplay of design, implementation, and context. Successful reforms require not only robust federal frameworks but also state-level buy-in and mechanisms to address affordability and accessibility. By studying past successes and failures, policymakers can craft evidence-based solutions that sustainably reduce the number of uninsured Americans, ensuring that coverage remains a right rather than a privilege.
Understanding Insurance: Key Basic Characteristics Every Policyholder Should Know
You may want to see also
Frequently asked questions
As of the latest data (2023), approximately 8-10% of Americans, or around 26-30 million people, are uninsured.
The primary reasons include high insurance costs, lack of employer-sponsored coverage, and ineligibility for public programs like Medicaid or Medicare.
The number has fluctuated; it decreased significantly after the Affordable Care Act (ACA) but has seen slight increases in recent years due to factors like policy changes and economic shifts.
States like Texas, Florida, and Georgia consistently report higher uninsured rates, often due to stricter Medicaid eligibility criteria and lower enrollment in ACA marketplace plans.