In the United States, the issue of health insurance coverage remains a significant concern, with millions of Americans lacking access to essential healthcare services. Despite efforts to expand coverage through initiatives like the Affordable Care Act, a substantial portion of the population remains uninsured due to factors such as high premiums, limited employer-sponsored plans, and gaps in public programs like Medicaid. Understanding the scope of this problem is crucial, as it highlights disparities in access to care, financial burdens on individuals and families, and broader implications for public health and economic stability. Examining the number of uninsured Americans sheds light on the ongoing challenges in achieving universal healthcare coverage in the nation.
Explore related products






What You'll Learn
![]()
Uninsured rates by state
As of the latest data, Texas leads the nation with the highest uninsured rate, hovering around 18%, significantly above the national average of approximately 9%. This disparity highlights the stark differences in healthcare access across states, influenced by factors such as Medicaid expansion, state policies, and economic conditions. For instance, Texas’s decision not to expand Medicaid under the Affordable Care Act has left a substantial portion of its low-income population without coverage. In contrast, states like Massachusetts and Vermont boast uninsured rates below 3%, thanks to comprehensive state-level healthcare initiatives and broader Medicaid eligibility criteria.
Analyzing these variations reveals a clear pattern: states that have expanded Medicaid tend to have lower uninsured rates. For example, California, which embraced Medicaid expansion early, has reduced its uninsured rate to around 7%. Conversely, states like Florida and Georgia, which have not expanded Medicaid, struggle with uninsured rates exceeding 12%. This divide underscores the critical role of policy decisions in shaping healthcare access. Policymakers in states with high uninsured rates could look to successful models like Massachusetts’s near-universal coverage system, which combines Medicaid expansion with a state-run health insurance marketplace.
For individuals living in states with high uninsured rates, practical steps can mitigate the lack of coverage. First, explore federally funded community health centers, which offer sliding-scale fees based on income. Second, utilize the Health Insurance Marketplace during open enrollment to find affordable plans, especially if your income qualifies for premium tax credits. Third, check eligibility for state-specific programs or subsidies, as some states offer additional assistance beyond federal options. For example, New York’s Essential Plan provides low-cost coverage to residents earning up to 200% of the federal poverty level.
A comparative analysis of uninsured rates by state also reveals demographic disparities. In states like Mississippi, where the uninsured rate is around 13%, rural populations face greater challenges due to limited healthcare infrastructure. Urban areas in states like Texas, despite higher overall uninsured rates, often have more resources and safety-net hospitals. Addressing these disparities requires targeted solutions, such as expanding telehealth services in rural areas and increasing funding for urban safety-net providers. States with lower uninsured rates, like Hawaii, demonstrate the effectiveness of combining robust public health systems with employer-based coverage mandates.
Finally, the takeaway is clear: uninsured rates are not just a national issue but a state-specific challenge shaped by local policies and demographics. States with the lowest uninsured rates provide a roadmap for others—expand Medicaid, invest in public health infrastructure, and create accessible insurance marketplaces. For residents in high-uninsured states, proactive steps like exploring all coverage options and advocating for policy change can make a difference. As the healthcare landscape evolves, understanding these state-level variations is essential for both policymakers and individuals seeking to improve access to care.
Unveiling the Oddities: Who Are These Weird Homeowner Insurance Companies?
You may want to see also
Explore related products






![]()
Impact of income on coverage
Income is a critical determinant of health insurance coverage in the United States, with a stark divide between higher and lower earners. According to the U.S. Census Bureau, in 2022, 8.5% of Americans were uninsured, but this rate varies dramatically by income level. Among households earning below the federal poverty level (FPL), approximately 20% lack coverage, compared to just 4% of those earning 400% above the FPL or more. This disparity highlights how financial constraints directly limit access to healthcare, even with programs like Medicaid designed to bridge the gap.
Consider the mechanics of this relationship: lower-income individuals often face a Catch-22. While Medicaid expansion under the Affordable Care Act (ACA) aimed to cover those earning up to 138% of the FPL, 11 states have yet to adopt it, leaving millions in the "coverage gap"—earning too much for traditional Medicaid but too little for ACA subsidies. For example, a single adult earning $13,000 annually in Texas falls into this gap, unable to afford private insurance premiums averaging $456 per month. Even for those eligible for subsidies, out-of-pocket costs like deductibles ($4,800 on average for a Bronze plan) remain prohibitive.
The impact of income on coverage extends beyond premiums to broader health outcomes. A 2021 study in *Health Affairs* found that uninsured low-income adults are 40% less likely to receive preventive care, such as cancer screenings, compared to their insured peers. This delay in care often leads to more severe—and costly—health issues down the line. For instance, untreated hypertension in a 45-year-old uninsured worker can escalate to a heart attack by age 55, incurring $100,000 in emergency care costs, compared to $500 annually for preventive medication.
To mitigate these disparities, targeted interventions are essential. Employers can play a role by offering health savings accounts (HSAs) or flexible spending arrangements (FSAs) to help workers manage costs. Policymakers should prioritize closing the Medicaid gap and capping out-of-pocket expenses at 5% of income for subsidized plans. Individuals can explore local clinics offering sliding-scale fees or programs like Ryan White for HIV/AIDS care. For example, a family of four earning $30,000 annually might qualify for a Silver plan with a $200 monthly premium and a $1,000 deductible through Healthcare.gov, a more manageable option than going uninsured.
Ultimately, the link between income and coverage underscores the need for systemic solutions. While incremental steps like expanding subsidies or employer-based programs help, they are band-aids on a deeper wound. Until healthcare is decoupled from income, millions will continue to face impossible choices between paying for insurance and meeting basic needs. The takeaway is clear: addressing affordability requires not just policy reform but a reimagining of how we fund and deliver care in America.
Why Insurance Companies Require Your SSN: Understanding the Necessity
You may want to see also
Explore related products






![]()
Role of employer-based insurance
Employer-based insurance covers approximately 155 million Americans, making it the largest source of health coverage in the U.S. This system, where employers subsidize or fully fund health plans for employees, emerged during World War II as a workaround to wage freezes. Today, it remains a cornerstone of the American healthcare system, though its reach is uneven. For instance, only 52% of workers in firms with fewer than 50 employees have access to employer-sponsored insurance, compared to 90% in larger firms. This disparity highlights the system’s limitations, particularly for low-wage and part-time workers.
The structure of employer-based insurance creates a paradox: it ties health coverage to employment, which can both stabilize access for some and exclude others. For full-time workers in stable jobs, this system often provides comprehensive coverage at a fraction of the cost of individual plans. However, job loss or transition can lead to gaps in coverage, as seen during economic downturns. For example, during the 2008 recession, an estimated 2.6 million non-elderly Americans lost employer-sponsored insurance. This volatility underscores the system’s reliance on economic conditions, leaving vulnerable populations at risk.
From a policy perspective, employer-based insurance complicates efforts to achieve universal coverage. While it reduces the burden on public programs like Medicaid, it also fragments the insurance market. Employers negotiate plans with varying benefits, creating inconsistencies in care quality and cost. For instance, a study by the Kaiser Family Foundation found that annual premiums for family coverage in 2023 averaged $23,968, with employees contributing $6,575. This financial strain on workers, coupled with the system’s exclusion of gig workers and small-business employees, fuels debates about alternative models, such as a single-payer system or expanded public options.
Practical steps to mitigate the limitations of employer-based insurance include expanding access to Affordable Care Act (ACA) marketplaces for those without employer coverage and incentivizing small businesses to offer health plans. For individuals, understanding COBRA continuation coverage—which allows temporary extension of employer-based insurance after job loss—can provide a bridge during transitions. Additionally, advocating for policies that decouple health insurance from employment could reduce systemic vulnerabilities. As the workforce evolves with more gig and part-time roles, reevaluating this decades-old model is essential to ensuring broader, more equitable coverage.
Renewing Your Health Insurance: A Step-by-Step Guide to Seamless Coverage
You may want to see also
Explore related products



$14.77 $18



![]()
Medicaid and CHIP enrollment
As of 2023, approximately 8.5% of Americans, or about 28 million people, lack health insurance. This figure, while lower than pre-Affordable Care Act (ACA) levels, still highlights significant gaps in coverage. Among the insured, Medicaid and the Children’s Health Insurance Program (CHIP) play a critical role, covering over 80 million individuals, including low-income adults, children, pregnant women, and people with disabilities. Understanding Medicaid and CHIP enrollment is essential to addressing the uninsured rate, as these programs serve as a safety net for vulnerable populations.
Eligibility and Enrollment Process
Medicaid and CHIP eligibility varies by state but generally targets households with incomes up to 138% of the federal poverty level (FPL) for adults and higher thresholds for children. For example, in 2023, a family of four earning up to $38,295 may qualify for Medicaid in states that expanded the program under the ACA. CHIP extends coverage to children in families earning too much for Medicaid but still below 200% of the FPL, roughly $56,310 for a family of four. Enrollment typically occurs through state-run marketplaces or healthcare.gov, with year-round applications for those qualifying under Medicaid’s continuous enrollment provisions. Practical tip: Use the “Am I Eligible?” tool on healthcare.gov to check qualifications before applying.
Impact of Continuous Enrollment Unwinding
The COVID-19 public health emergency (PHE) allowed for continuous Medicaid enrollment, preventing disenrollment regardless of eligibility changes. However, this policy ended in April 2023, triggering a massive unwinding process. States are now redetermining eligibility for all enrollees, with projections that up to 15 million people could lose coverage, many due to procedural reasons rather than ineligibility. This shift underscores the importance of updating contact information and promptly responding to renewal notices. Caution: Failure to complete renewal paperwork can result in coverage gaps, even for those still eligible.
Comparative Benefits of Medicaid and CHIP
Medicaid and CHIP offer comprehensive benefits tailored to their populations. Medicaid covers a broad range of services, including hospital stays, doctor visits, and long-term care, with minimal out-of-pocket costs. CHIP focuses on pediatric care, including immunizations, dental, and vision services, often with no premiums or low copays. For instance, CHIP ensures children receive age-appropriate preventive care, such as annual well-child visits and developmental screenings. Comparative analysis shows these programs reduce health disparities by providing access to care that might otherwise be unaffordable for low-income families.
Strategies to Maximize Enrollment
To address coverage gaps, states and advocates are employing targeted strategies. Outreach campaigns in underserved communities, simplified application processes, and partnerships with schools and community organizations are proving effective. For example, some states use school lunch program data to identify potentially eligible children for CHIP. Additionally, extending postpartum Medicaid coverage from 60 days to 12 months, as adopted by several states, addresses maternal health disparities. Persuasive takeaway: Expanding these efforts could significantly reduce the uninsured rate, particularly among children and pregnant women, by ensuring eligible individuals are aware of and enrolled in available programs.
Step-by-Step Guide to Enrolling in USPS Health Insurance Benefits
You may want to see also
Explore related products

$8.27 $12.99





![]()
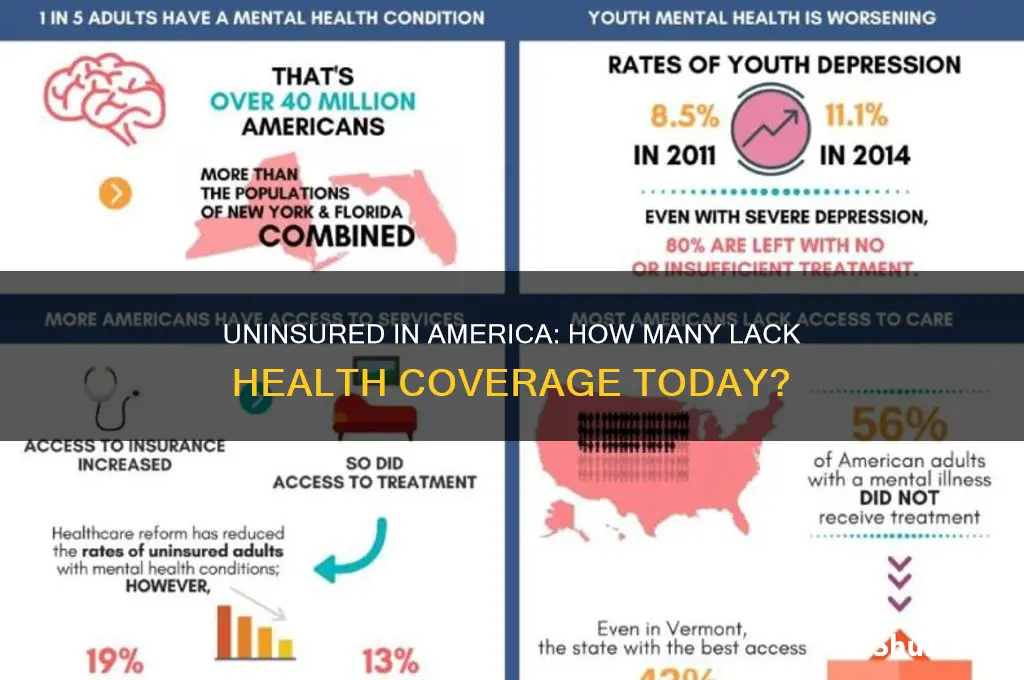
Uninsured demographics (age, race, etc.)
The uninsured rate in the United States isn’t uniform—it varies sharply by age, race, income, and geography. Young adults aged 19 to 34 are disproportionately uninsured, with rates nearly double those of older adults. This group often faces financial instability, part-time employment, or jobs without benefits, making health insurance unaffordable or inaccessible. For example, 14.3% of adults aged 19 to 25 lacked coverage in 2022, compared to 7.8% of those aged 50 to 64. Understanding these age-based disparities is critical for tailoring solutions, such as expanding Medicaid or offering subsidized plans for this demographic.
Racial and ethnic disparities in uninsured rates reveal systemic inequities. Hispanic Americans have the highest uninsured rate at 19.1%, followed by Native Americans at 16.6%. In contrast, only 5.9% of non-Hispanic whites lack coverage. These gaps persist due to factors like lower income levels, employment in industries without benefits, and immigration status barriers. For instance, undocumented immigrants are ineligible for Medicaid or Affordable Care Act (ACA) subsidies, leaving them with limited options. Addressing these disparities requires culturally sensitive policies, such as language-accessible enrollment processes and targeted outreach in underserved communities.
Income is a defining factor in insurance status, with poverty as a primary driver of uninsurance. Households earning below the federal poverty level (FPL) are three times more likely to be uninsured than those earning above 400% of the FPL. States that expanded Medicaid under the ACA saw significant reductions in uninsured rates among low-income populations, but 10 states still haven’t expanded, leaving millions in the "coverage gap"—earning too much for Medicaid but too little for ACA subsidies. Practical steps to mitigate this include advocating for Medicaid expansion and simplifying enrollment processes to reduce administrative barriers.
Geography plays a surprising role in uninsured rates, with Southern states consistently topping the list. Texas, for example, has an uninsured rate of 18.4%, while Massachusetts boasts just 3.3%. This variation stems from state-level policy decisions, such as Medicaid expansion and investment in public health infrastructure. Rural areas face additional challenges, including fewer healthcare providers and limited access to insurance navigators. To combat this, policymakers could incentivize providers to serve rural areas and expand telehealth services, ensuring coverage isn’t just a privilege of urban living.
Finally, employment status is a critical determinant of insurance coverage. Part-time workers and those in gig economy jobs are far less likely to receive employer-sponsored insurance, which covers 54.4% of Americans. Small businesses, which employ nearly half of the private-sector workforce, are less likely to offer health benefits due to cost constraints. Freelancers and self-employed individuals often face prohibitively expensive individual market plans. Solutions include expanding access to ACA marketplace plans, offering tax credits for small businesses to provide insurance, and exploring portable benefit models that move with workers across jobs.
Top Insurance Partners of Copart: A Comprehensive Guide
You may want to see also
Frequently asked questions
As of 2023, approximately 8% of Americans, or around 27 million people, do not have health insurance, according to the U.S. Census Bureau.
The primary reasons include high insurance costs, lack of employer-sponsored coverage, ineligibility for public programs like Medicaid, and gaps in state policies, such as not expanding Medicaid under the Affordable Care Act.
The number of uninsured Americans has fluctuated over the years. It reached a low of around 26 million in 2016 due to the Affordable Care Act but has since risen slightly due to factors like policy changes and economic shifts.
Low-income individuals, young adults, people of color, and those living in states that did not expand Medicaid are disproportionately more likely to be uninsured. Additionally, workers in part-time or gig economy jobs often lack access to employer-sponsored insurance.