The lack of health insurance in the United States has profound and often devastating consequences, contributing to a significant number of preventable deaths each year. Studies estimate that tens of thousands of Americans die annually due to inadequate access to healthcare, a direct result of being uninsured. Without insurance, individuals often delay or forgo necessary medical treatments, screenings, and medications, leading to untreated chronic conditions, late-stage diagnoses, and avoidable complications. This disparity disproportionately affects low-income and marginalized communities, exacerbating existing health inequities. Addressing the issue of uninsured individuals is not only a matter of public health but also a critical step toward ensuring social justice and reducing preventable mortality in the U.S.
| Characteristics | Values |
|---|---|
| Annual Deaths Due to Lack of Health Insurance (US) | Approximately 45,000 (as of latest studies, e.g., 2022 estimates) |
| Primary Causes of Death | Preventable conditions like heart disease, cancer, diabetes, and infections |
| Demographic Most Affected | Low-income individuals, racial/ethnic minorities, and young adults |
| Financial Impact | Uninsured individuals are 25% more likely to die prematurely |
| Geographic Disparity | Higher death rates in states without Medicaid expansion |
| Comparative Statistic | Lack of insurance is linked to nearly 30% higher mortality risk |
| Policy Impact | Medicaid expansion reduces mortality rates by 6% in eligible populations |
| Source of Data | Studies from The Lancet, American Journal of Public Health, and Commonwealth Fund |
| Year of Latest Data | 2022-2023 |
Explore related products






What You'll Learn
![]()
Annual uninsured death toll
Each year, an estimated 30,000 Americans die prematurely due to lack of health insurance. This staggering number, derived from a 2009 study by the American Journal of Public Health, remains a stark reminder of the human cost of an uninsured population. The study, which analyzed data from the National Health and Nutrition Examination Survey, found that uninsured adults were 40% more likely to die prematurely than their insured counterparts. This translates to roughly 82 preventable deaths every day, a silent epidemic that disproportionately affects low-income individuals and communities of color.
To put this into perspective, consider the impact on specific age groups. Young adults aged 18-24, often caught in the gap between parental coverage and employer-sponsored plans, face a heightened risk. Without insurance, they may delay seeking care for conditions like diabetes or hypertension, leading to complications that could have been managed with early intervention. Similarly, older adults nearing retirement age, who haven't yet qualified for Medicare, are vulnerable. A 60-year-old without insurance is less likely to receive timely screenings for cancer or heart disease, reducing their chances of survival.
The annual uninsured death toll isn't just a statistic; it's a call to action. Policymakers can address this crisis by expanding Medicaid eligibility, as seen in states that adopted the Affordable Care Act's Medicaid expansion. This simple policy change has been linked to a 6% reduction in mortality rates among low-income adults. Employers can also play a role by offering affordable health plans to part-time workers, who are often excluded from company-sponsored insurance. For individuals, understanding enrollment periods and available subsidies is crucial. The Healthcare Marketplace, for instance, offers plans with premiums as low as $10/month for those earning up to 150% of the federal poverty level.
Comparing the US to other high-income countries highlights the urgency of this issue. Nations with universal healthcare systems, such as Canada and the UK, report significantly lower rates of preventable deaths. In Canada, where healthcare is publicly funded, the annual preventable death rate is nearly half that of the US. This disparity underscores the need for systemic change. While incremental reforms can help, a comprehensive solution requires addressing the root causes of uninsurance: high costs, limited access, and fragmented coverage. Until then, the annual uninsured death toll will remain a grim testament to the consequences of an inequitable healthcare system.
Geico's Medical Insurance: What You Need to Know
You may want to see also
Explore related products






![]()
Preventable deaths without coverage
Each year, an estimated 30,000 preventable deaths occur in the United States due to lack of health insurance. This staggering number highlights a stark reality: without coverage, individuals often delay or forgo necessary medical care, turning treatable conditions into fatal ones. For instance, a person with undiagnosed hypertension might not receive the medication and lifestyle guidance needed to manage their condition, increasing their risk of heart attack or stroke. Similarly, early-stage cancers, when detected and treated promptly, have high survival rates, but without insurance, many go undetected until it’s too late. These deaths are not merely statistics; they represent lives cut short due to systemic barriers to care.
Consider the case of a 45-year-old uninsured individual experiencing persistent chest pain. Without insurance, they might avoid seeking medical attention due to the prohibitive cost of emergency room visits or diagnostic tests. This delay can turn a manageable condition, like angina, into a fatal heart attack. Research shows that uninsured adults are 25% more likely to die prematurely than their insured counterparts, largely due to such scenarios. Even routine preventive measures, like cholesterol screenings or diabetes monitoring, become inaccessible without coverage, allowing preventable complications to escalate unchecked.
From a comparative perspective, countries with universal healthcare systems report significantly lower rates of preventable deaths. For example, the United Kingdom, with its National Health Service, ensures that individuals receive timely care regardless of their financial situation. In contrast, the U.S. system often ties healthcare access to employment or income, leaving millions vulnerable. A study published in *The Lancet* found that expanding Medicaid coverage reduced mortality rates by 6% in states that adopted the expansion, underscoring the life-saving potential of accessible healthcare.
To address this crisis, practical steps must be taken. First, policymakers should prioritize expanding Medicaid in all states, ensuring low-income individuals have access to essential care. Second, employers can play a role by offering affordable health insurance options to workers, particularly in industries with high uninsured rates, such as food service and construction. Individuals can also take proactive measures, like utilizing community health clinics or seeking out sliding-scale fee programs for basic care. While these steps are not a complete solution, they can mitigate the risk of preventable deaths until systemic changes are implemented.
Ultimately, the 30,000 preventable deaths annually are a call to action. They underscore the moral and practical imperative of ensuring healthcare access for all. By addressing the root causes of uninsured rates and implementing targeted interventions, society can reduce this tragic toll and move toward a healthier, more equitable future.
Kaiser Permanente: Can I Access Services Without Insurance?
You may want to see also
Explore related products






![]()
Impact on chronic conditions
Uninsured individuals with chronic conditions face a stark reality: their lack of coverage often translates to delayed diagnoses, inadequate treatment, and poorer health outcomes. This vulnerability is particularly pronounced in conditions like diabetes, hypertension, and asthma, where consistent monitoring and medication adherence are critical. Without insurance, routine check-ups, lab tests, and prescription medications become unaffordable luxuries, leading to complications that could have been prevented with timely intervention.
Consider diabetes, a condition affecting over 37 million Americans. For uninsured patients, the cost of glucose monitors, insulin, and regular A1C tests can be prohibitive. A study by the American Diabetes Association found that uninsured adults with diabetes are twice as likely to experience uncontrolled blood sugar levels compared to their insured counterparts. This increases the risk of severe complications such as kidney failure, heart disease, and amputations. For instance, a 45-year-old uninsured diabetic might skip insulin doses to stretch their supply, leading to a diabetic coma—a preventable crisis with proper access to care.
Hypertension, another prevalent chronic condition, similarly suffers from the absence of insurance. Without coverage, patients often forgo blood pressure medications like lisinopril or amlodipine, which cost upwards of $50 per month without subsidies. This neglect can lead to strokes, heart attacks, or renal failure. A 2020 study in *Circulation* revealed that uninsured individuals with hypertension are 50% more likely to experience cardiovascular events than those with insurance. Practical steps, such as community health clinics offering discounted medications or home blood pressure monitoring, can mitigate some risks, but these solutions are often insufficient without systemic support.
Asthma, a chronic respiratory condition, highlights another dimension of this crisis. Inhalers like albuterol or Advair, essential for managing asthma attacks, can cost over $200 without insurance. Uninsured patients may ration their medication, increasing the likelihood of severe asthma attacks requiring emergency care. Children are particularly vulnerable; a 2018 study in *Pediatrics* found that uninsured children with asthma are three times more likely to be hospitalized than insured children. Schools and community programs can provide emergency inhalers, but this does not replace the need for consistent, affordable care.
The takeaway is clear: the absence of health insurance exacerbates the challenges of managing chronic conditions, turning manageable diseases into life-threatening ones. While stopgap measures like community clinics or medication assistance programs offer temporary relief, they are no substitute for comprehensive coverage. Policymakers, healthcare providers, and advocates must prioritize expanding access to insurance and affordable care to prevent unnecessary suffering and deaths among the uninsured.
Unlock Free Health Insurance: A Step-by-Step Application Guide
You may want to see also
Explore related products






![]()
Financial barriers to care
In the United States, an estimated 45,000 deaths annually are attributed to lack of health insurance, a stark reminder of the lethal consequences of financial barriers to care. This figure, derived from studies analyzing mortality rates among uninsured populations, underscores the systemic inequities embedded in the healthcare system. Financial barriers not only delay access to preventive services but also force individuals to forgo essential treatments, turning manageable conditions into fatal ones. For instance, uninsured adults are 25% more likely to die prematurely than their insured counterparts, often due to untreated chronic illnesses like diabetes or hypertension.
Consider the case of a 45-year-old uninsured individual diagnosed with early-stage breast cancer. Without insurance, the out-of-pocket cost for diagnostic imaging, surgery, and chemotherapy can exceed $100,000. Faced with such prohibitive expenses, many delay or abandon treatment altogether. This delay transforms a highly treatable condition—with a 90% five-year survival rate when caught early—into a terminal diagnosis. Such scenarios are not anomalies; they reflect the harsh reality for millions who cannot afford coverage.
Financial barriers also manifest in the form of high deductibles and copays, even among the insured. A Commonwealth Fund study found that 44% of underinsured adults (those with inadequate coverage) skipped necessary care due to cost. For example, a $50 copay for a specialist visit or a $500 deductible for emergency care can deter low-income individuals from seeking timely intervention. This "underinsurance" phenomenon blurs the line between having coverage and accessing care, effectively trapping individuals in a cycle of financial vulnerability.
To mitigate these barriers, policymakers and healthcare providers must adopt targeted interventions. Expanding Medicaid eligibility, as seen in states like California and New York, has reduced uninsured rates and improved health outcomes. Additionally, implementing sliding-scale fee structures for low-income patients can make care more affordable. For instance, a clinic in Texas offers $20 primary care visits for uninsured patients earning below 200% of the federal poverty level, significantly increasing access. Such models demonstrate that financial barriers, while daunting, are not insurmountable.
Ultimately, the human cost of financial barriers to care demands urgent action. Every preventable death is a failure of the system, a reminder that healthcare is not a privilege but a fundamental right. By addressing affordability through policy reforms and innovative payment models, society can move closer to ensuring that no one dies simply because they cannot afford care. The question is not whether we can afford to act, but whether we can afford the moral and economic consequences of inaction.
Medical Insurance: Quitting Your Job, Not Your Coverage
You may want to see also
Explore related products


![]()
Demographics most affected
The lack of health insurance in the U.S. disproportionately impacts specific demographic groups, leading to higher mortality rates and exacerbated health disparities. Among these, low-income individuals are the hardest hit. Studies show that adults in households earning below 200% of the federal poverty level face significantly higher uninsured rates compared to higher-income counterparts. This financial barrier often delays or prevents access to preventive care, early disease detection, and timely treatment, contributing to preventable deaths. For instance, uninsured low-income individuals are 40% more likely to die from conditions like diabetes or heart disease due to inadequate management.
Another critically affected demographic is racial and ethnic minorities, particularly Black and Hispanic populations. Structural inequities, including systemic racism and limited access to employer-sponsored insurance, leave these groups with higher uninsured rates. Black Americans, for example, are 1.5 times more likely to be uninsured than their white peers, while Hispanic individuals account for nearly a third of the uninsured population despite representing 18% of the total U.S. population. These disparities translate into higher mortality rates from treatable conditions like hypertension, where uninsured Black adults are 20% more likely to experience fatal complications compared to insured individuals.
Young adults, aged 18–34, also face heightened risks due to lack of insurance, often caught in the gap between parental coverage and employer-provided plans. This age group constitutes nearly 30% of the uninsured population, with many forgoing coverage due to perceived good health or cost concerns. However, this demographic is not immune to accidents, mental health crises, or undiagnosed chronic conditions. For example, uninsured young adults are twice as likely to die from opioid overdoses or untreated infections compared to their insured peers, highlighting the lethal consequences of delayed care.
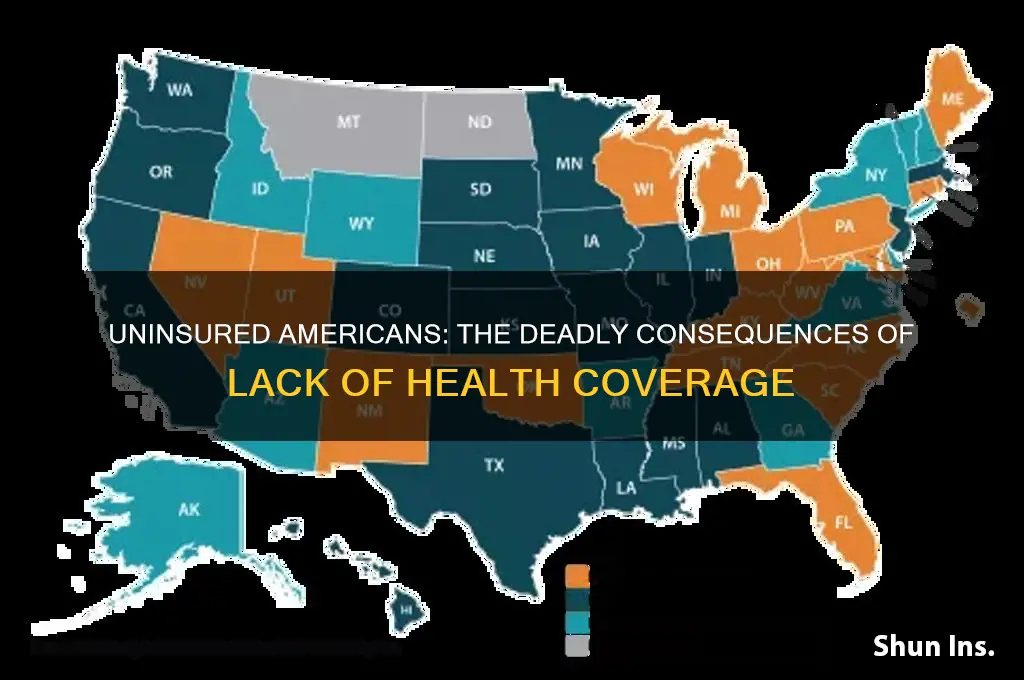
Lastly, residents of states that have not expanded Medicaid under the Affordable Care Act (ACA) face a unique vulnerability. In these states, an estimated 2.2 million people fall into the "coverage gap," earning too much to qualify for traditional Medicaid but too little to afford private insurance. This gap disproportionately affects rural and Southern states, where uninsured rates are 30% higher than in expansion states. For instance, in Texas, where Medicaid expansion has not been adopted, uninsured rates among low-income adults are 27%, compared to 8% in expansion states like California. This policy-driven disparity results in thousands of preventable deaths annually, particularly from conditions like cancer, where early detection rates are 50% lower among the uninsured.
To address these disparities, targeted interventions are essential. Expanding Medicaid in non-expansion states could immediately cover 4 million uninsured adults, reducing mortality rates by an estimated 15%. Additionally, subsidizing premiums for low-income individuals and increasing enrollment assistance for young adults and minorities could bridge coverage gaps. Employers can play a role by offering affordable plans, while policymakers must address systemic barriers like language access and immigration status that deter enrollment. Without such measures, the demographics most affected will continue to bear the brunt of a system that ties health outcomes to insurance status.
Top Insurance Companies Offering the Best Value for Your Money
You may want to see also
Frequently asked questions
Studies estimate that approximately 30,000 to 45,000 people die annually in the US due to lack of health insurance, as they often delay or forgo necessary medical care.
Uninsured individuals often face delayed diagnosis, lack of preventive care, inability to afford medications, and limited access to timely treatment, leading to preventable deaths.
Lack of health insurance is a significant contributor to mortality, comparable to other risk factors like obesity and smoking, particularly for treatable conditions like heart disease and cancer.
Yes, low-income individuals, racial and ethnic minorities, and those in states without Medicaid expansion are disproportionately affected by deaths related to lack of health insurance.
Yes, studies show that expanding health insurance coverage, such as through Medicaid expansion, significantly reduces mortality rates by improving access to healthcare and preventive services.