The Democratic Republic of Congo (DRC) faces significant challenges in providing access to health insurance for its population. With a vast majority of its citizens living in poverty and a fragile healthcare system, the number of people with health insurance in the DRC remains alarmingly low. Estimates suggest that less than 5% of the population has any form of health coverage, leaving millions vulnerable to catastrophic health expenses and limited access to essential medical services. This lack of insurance exacerbates existing health disparities and hinders progress toward universal health coverage in the country.
| Characteristics | Values |
|---|---|
| Total Population (2023) | Approximately 102 million |
| Percentage with Health Insurance | Less than 5% (mostly limited to formal sector employees) |
| Urban vs. Rural Coverage | Higher in urban areas, negligible in rural areas |
| Public Health Insurance Coverage | Minimal; government schemes cover less than 2% of the population |
| Private Health Insurance Coverage | Very low, primarily for expatriates and high-income individuals |
| Out-of-Pocket Expenditure on Health | Over 70% of health spending is out-of-pocket |
| Access to Healthcare Facilities | Limited, especially in rural areas |
| Government Health Spending (2023) | Approximately 2-3% of GDP |
| Major Barriers to Insurance | Poverty, lack of awareness, weak healthcare infrastructure |
| International Aid Dependency | Significant reliance on international donors for healthcare funding |
| Recent Initiatives | Efforts to expand community-based health insurance schemes |
Explore related products






What You'll Learn
- Urban vs. Rural Coverage: Compare health insurance rates between urban and rural populations in the DRC
- Public vs. Private Insurance: Analyze the prevalence of public versus private health insurance options in the DRC
- Income and Access: Examine how household income levels impact access to health insurance in the DRC
- Government Health Policies: Assess the role of DRC government policies in promoting health insurance coverage
- Regional Disparities: Investigate health insurance coverage differences across provinces or regions in the DRC
![]()
Urban vs. Rural Coverage: Compare health insurance rates between urban and rural populations in the DRC
In the Democratic Republic of Congo (DRC), health insurance coverage is starkly divided along urban and rural lines, with urban populations benefiting from significantly higher access compared to their rural counterparts. This disparity is rooted in the concentration of healthcare infrastructure and economic opportunities in cities like Kinshasa and Lubumbashi, where formal employment—a primary pathway to insurance—is more prevalent. Rural areas, comprising over 60% of the DRC’s population, often rely on subsistence farming and lack access to formal healthcare systems, let alone insurance schemes.
Consider the logistical challenges in rural DRC: vast distances separate villages from healthcare facilities, and many regions lack reliable transportation networks. Even when health insurance options exist, rural residents face barriers such as low literacy rates, limited awareness of insurance benefits, and inability to afford premiums. For instance, community-based health insurance (CBHI) schemes, which are more feasible in rural settings, cover less than 5% of the rural population due to insufficient funding and administrative hurdles. In contrast, urban workers in sectors like mining or government services often receive employer-sponsored insurance, though this still excludes the large informal sector workforce.
To bridge this gap, policymakers must adopt targeted strategies. In rural areas, expanding CBHI programs by subsidizing premiums for low-income households and integrating them with mobile money platforms could increase enrollment. Urban initiatives should focus on extending coverage to informal workers, who constitute over 80% of the urban labor force, through microinsurance products tailored to their income levels. For example, a pilot program in Kinshasa offering pay-as-you-go health insurance via mobile phones saw a 25% uptake among street vendors within six months.
A cautionary note: simply increasing insurance availability won’t address underlying healthcare disparities. Rural facilities often lack essential medicines and trained staff, rendering insurance less valuable. Pairing insurance expansion with investments in rural health infrastructure—such as equipping clinics and training community health workers—is critical. Urban areas, meanwhile, must tackle the fragmentation of insurance providers to ensure seamless access to services.
In conclusion, addressing the urban-rural health insurance divide in the DRC requires a dual approach: making insurance more accessible and affordable in rural areas while ensuring urban coverage reaches the informal sector. Without such measures, the majority of the DRC’s population will remain uninsured, perpetuating cycles of poverty and ill health. Practical steps, from leveraging technology to strengthening healthcare systems, can turn this disparity into an opportunity for equitable progress.
Medicare and Insurance Agencies: How They Work Together
You may want to see also
Explore related products






![]()
Public vs. Private Insurance: Analyze the prevalence of public versus private health insurance options in the DRC
In the Democratic Republic of Congo (DRC), the health insurance landscape is starkly divided, with public options struggling to meet demand and private alternatives remaining inaccessible to most. Public health insurance, primarily through the National Health Insurance Fund (CNAM), covers less than 5% of the population, largely limited to formal sector employees and their dependents. This leaves the vast majority—over 90%—without any formal coverage, relying instead on out-of-pocket payments or traditional healing practices. Private insurance, though growing, is concentrated in urban areas like Kinshasa and Lubumbashi, catering to expatriates and the affluent elite. The disparity highlights a system where public initiatives are underfunded and fragmented, while private solutions exacerbate inequities.
To understand this divide, consider the structural challenges. The DRC’s public health system is chronically underfunded, with government spending on health hovering around 3% of GDP, far below the WHO-recommended 5%. This limits CNAM’s capacity to expand coverage, even as it faces administrative inefficiencies and corruption. Private insurers, on the other hand, operate in a largely unregulated market, offering plans that cost upwards of $500 annually—an unattainable sum for the average Congolese earning less than $2 per day. The result is a dual system: one where public insurance is theoretically universal but practically exclusive, and private insurance is a luxury few can afford.
A comparative analysis reveals the consequences of this imbalance. In neighboring Rwanda, community-based health insurance (CBHI) covers over 80% of the population, demonstrating the potential for public-led initiatives in low-resource settings. The DRC’s failure to replicate such models underscores the need for policy reforms that prioritize affordability and accessibility. Private insurers could play a role by offering tiered plans or partnering with employers, but without regulatory oversight, such solutions risk deepening disparities. The takeaway is clear: bridging the gap requires a hybrid approach, leveraging public funding and private innovation while addressing systemic barriers.
For those navigating this landscape, practical steps can mitigate risks. Formal sector workers should verify CNAM enrollment through their employers, ensuring dependents are included. Informal workers and rural residents, who constitute 80% of the population, should explore community health cooperatives or mutual health organizations (MHOs), which pool resources for shared coverage. While not insurance in the traditional sense, these models offer a safety net in emergencies. For the affluent, private plans from companies like Activa Assurances or Sonas provide comprehensive coverage but require careful review of exclusions and network limitations. Ultimately, the DRC’s insurance dilemma demands collective action, but individuals can still take incremental steps toward protection.
Did Hillary Clinton Create the Children's Health Insurance Program?
You may want to see also
Explore related products






![]()
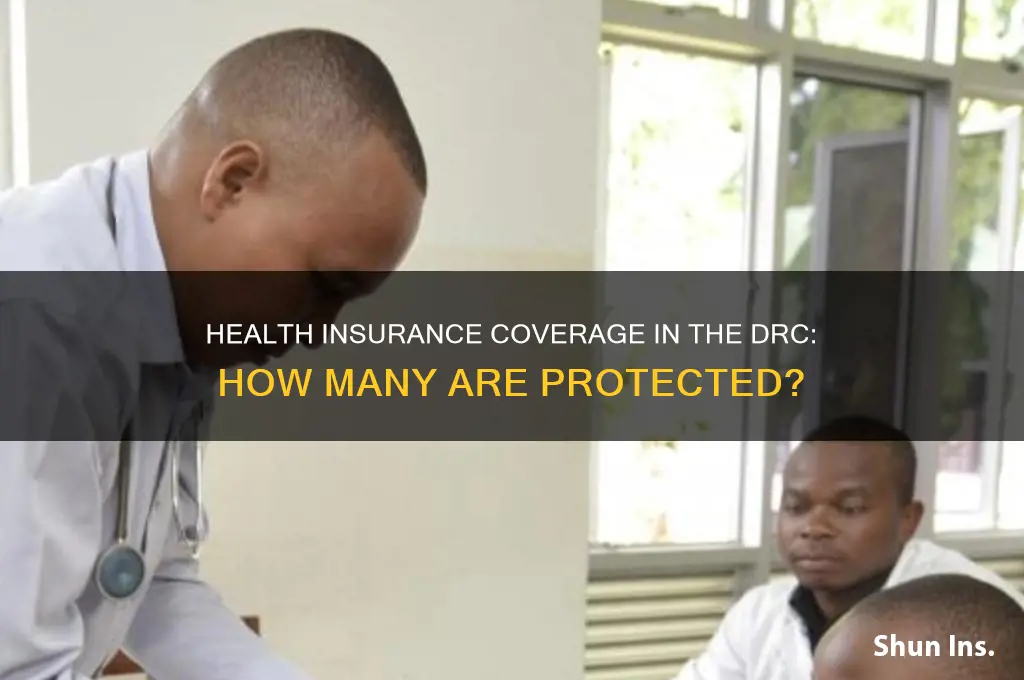
Income and Access: Examine how household income levels impact access to health insurance in the DRC
In the Democratic Republic of Congo (DRC), household income levels serve as a critical determinant of access to health insurance, with stark disparities between the wealthy and the impoverished. Data reveals that less than 5% of the population has any form of health insurance, and this coverage is predominantly concentrated among the top 10% of income earners. For the majority living on less than $2 a day, health insurance remains an unaffordable luxury. The informal economy, which employs over 80% of the workforce, offers no employer-based insurance options, leaving low-income households to rely on out-of-pocket payments or community health schemes, which are often insufficient and unreliable.
Analyzing the income-access nexus, it becomes evident that the cost of health insurance premiums in the DRC is prohibitively high for most households. A basic health insurance plan can cost upwards of $50 annually, a sum that represents nearly a month’s income for many families. This financial barrier is compounded by the lack of government subsidies or sliding-scale premiums that could make insurance more accessible to lower-income groups. Without targeted interventions, such as income-based premium reductions or public-private partnerships, the current system perpetuates a cycle where only the affluent can afford protection against catastrophic health expenses.
A comparative perspective highlights the role of policy in bridging the income-access gap. In neighboring Rwanda, community-based health insurance schemes cover over 90% of the population, largely due to government subsidies and low-cost premiums tailored to different income levels. The DRC, however, lacks such inclusive policies, leaving its health insurance landscape fragmented and exclusionary. Implementing a tiered premium system, where contributions are proportional to household income, could significantly improve access for low-income families while ensuring sustainability for insurers.
For practical guidance, households in the DRC can explore community health associations (mutuelles de santé) as a more affordable alternative to traditional insurance. These cooperatives pool resources from members to cover basic healthcare costs, with monthly contributions as low as $1 per person. While not comprehensive, they provide a safety net for routine medical needs. Additionally, families should prioritize preventive care, such as vaccinations and regular check-ups, to reduce the likelihood of costly treatments. Advocacy for policy reforms that address income disparities in health insurance access remains crucial for long-term systemic change.
In conclusion, the relationship between household income and health insurance access in the DRC is marked by profound inequities. Addressing this issue requires a multi-faceted approach, including affordable insurance options, government subsidies, and community-driven initiatives. Without such measures, the majority of the population will remain vulnerable to financial hardship in the face of health crises, perpetuating cycles of poverty and ill-health.
Understanding Visitor Medical Insurance Costs and Coverage
You may want to see also
Explore related products





![]()
Government Health Policies: Assess the role of DRC government policies in promoting health insurance coverage
The Democratic Republic of Congo (DRC) faces significant challenges in health insurance coverage, with estimates suggesting that less than 5% of the population has any form of health insurance. This stark reality underscores the critical need for effective government policies to bridge the gap between healthcare accessibility and financial protection. The DRC government’s role in promoting health insurance coverage is multifaceted, involving legislative frameworks, financial incentives, and public awareness campaigns. However, the success of these policies hinges on their implementation, sustainability, and alignment with the socio-economic realities of the population.
One of the primary mechanisms through which the DRC government has sought to expand health insurance coverage is the establishment of the National Health Insurance Fund (CNAM). Launched in 2016, CNAM aims to provide universal health coverage by pooling resources and subsidizing healthcare costs for vulnerable populations, including civil servants, formal sector workers, and eventually the informal sector. Despite its ambitious goals, CNAM’s impact has been limited by inadequate funding, administrative inefficiencies, and low enrollment rates. For instance, as of 2023, only a fraction of the targeted population has been enrolled, highlighting the need for stronger enforcement mechanisms and public trust-building initiatives.
To enhance the effectiveness of such policies, the DRC government must address systemic barriers that hinder health insurance uptake. These include the high cost of premiums relative to average incomes, lack of awareness about the benefits of health insurance, and a fragmented healthcare system that struggles to deliver quality services. A comparative analysis with countries like Rwanda, which has achieved over 80% health insurance coverage through community-based health insurance schemes, reveals the importance of tailoring policies to local contexts. For the DRC, this could mean prioritizing community-driven models that leverage existing social structures and are subsidized by both government and international donors.
Persuasively, the DRC government should also consider leveraging technology to streamline health insurance processes. Mobile money platforms, which are widely used in the DRC, could be integrated into premium payment systems to improve accessibility and reduce administrative costs. Additionally, public-private partnerships could play a pivotal role in expanding coverage, with private insurers offering affordable, tailored plans for different demographic groups. For example, introducing micro-insurance products for informal sector workers, who constitute the majority of the workforce, could significantly increase enrollment rates.
In conclusion, while the DRC government has taken steps to promote health insurance coverage through policies like CNAM, their impact remains limited by implementation challenges and systemic barriers. A more holistic approach, combining legislative reforms, financial innovations, and community engagement, is essential to achieve meaningful progress. By learning from successful models in other African countries and adapting them to the DRC’s unique context, the government can pave the way for a healthier, more financially secure population. Practical steps, such as subsidizing premiums for low-income groups and utilizing digital platforms for enrollment, could serve as immediate actionable measures to accelerate coverage expansion.
Switching Insurance for Better Medical Care for Your Family
You may want to see also
Explore related products


![]()
Regional Disparities: Investigate health insurance coverage differences across provinces or regions in the DRC
The Democratic Republic of Congo (DRC) is a vast country with significant regional variations in healthcare access, and health insurance coverage is no exception. A closer examination of provincial data reveals a stark divide, with urban centers like Kinshasa and Lubumbashi boasting relatively higher insurance penetration compared to rural provinces such as Maniema and Kasai. This disparity is not merely a statistical anomaly but a reflection of deeper socioeconomic and infrastructural inequalities.
Consider the following scenario: In Kinshasa, the capital city, approximately 15-20% of the population has some form of health insurance, primarily through employer-sponsored schemes or private providers. Contrast this with Maniema, where less than 2% of residents enjoy similar coverage. The reasons for this gap are multifaceted. Urban areas benefit from greater economic activity, higher concentrations of formal employment, and better access to healthcare facilities, all of which facilitate insurance uptake. Rural regions, on the other hand, are often characterized by subsistence agriculture, informal labor, and limited health infrastructure, making insurance both less accessible and less affordable.
To address these disparities, policymakers must adopt a targeted approach. For instance, in provinces like Kasai and Tanganyika, where health insurance coverage hovers around 3-5%, pilot programs could introduce community-based health insurance schemes. These initiatives, already successful in countries like Rwanda, pool resources at the local level to provide affordable coverage for essential health services. Additionally, leveraging mobile technology could extend insurance outreach in remote areas, where traditional banking and healthcare systems are underdeveloped.
However, implementing such solutions requires caution. Rural populations often face lower health literacy and may be skeptical of insurance schemes, perceiving them as unnecessary or unaffordable. Public awareness campaigns, tailored to local languages and cultural contexts, are essential to dispel misconceptions and build trust. Furthermore, ensuring transparency in premium collection and claims processing is critical to sustaining participation.
In conclusion, bridging the regional health insurance gap in the DRC demands a nuanced understanding of local dynamics and a commitment to inclusive strategies. By combining innovative solutions with community engagement, the DRC can move toward a more equitable healthcare system, where geography no longer dictates access to essential services.
Top Insurance Providers Offering Coverage in Protection 10 Zones
You may want to see also
Frequently asked questions
As of recent estimates, only a small fraction of the population in the DRC, approximately 5-10%, has access to formal health insurance, primarily through employer-based schemes or government programs.
The majority of the DRC population, around 80-90%, relies on out-of-pocket payments for healthcare due to the lack of widespread health insurance coverage.
Yes, the DRC has some government-funded health insurance programs, such as the National Health Insurance Scheme (CNAM), but coverage is limited and primarily benefits public sector employees.
The lack of health insurance leads to limited access to healthcare services, financial hardship for families, and reliance on traditional or informal healthcare providers, exacerbating health disparities.
Efforts include expanding community-based health insurance schemes, partnering with international organizations, and advocating for policy reforms to improve healthcare financing and accessibility.