The issue of uninsured Americans remains a pressing concern in the United States, with millions of citizens lacking access to adequate health coverage. Despite efforts to expand healthcare access, a significant portion of the population continues to face financial barriers to obtaining insurance, leaving them vulnerable to high medical costs and limited access to essential healthcare services. Understanding the scope of this problem is crucial, as it highlights disparities in healthcare access and underscores the need for ongoing policy reforms to ensure that all Americans have the opportunity to lead healthy lives.
Explore related products






What You'll Learn
![]()
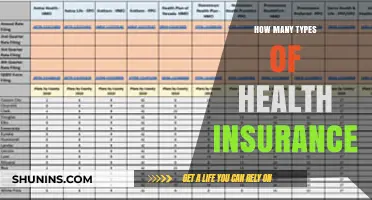
Uninsured rates by state
The uninsured rate in the United States varies significantly by state, reflecting disparities in healthcare access, economic conditions, and policy decisions. As of recent data, states like Texas and Florida consistently report higher uninsured rates, often exceeding 15% of their populations. In contrast, states such as Massachusetts and Vermont boast rates below 5%, largely due to their expansive Medicaid programs and state-level health insurance mandates. These differences highlight the impact of local policies on coverage outcomes.
Analyzing the trends, Southern and Western states often face higher uninsured rates due to factors like lower Medicaid expansion adoption and higher poverty levels. For instance, Texas, which has not expanded Medicaid under the Affordable Care Act, sees nearly 18% of its residents without insurance. Conversely, states that expanded Medicaid, such as California and New York, have seen significant reductions in uninsured rates, dropping to around 7% and 5%, respectively. This underscores the critical role of Medicaid expansion in closing coverage gaps.
For individuals living in states with high uninsured rates, practical steps can make a difference. First, explore state-specific health insurance marketplaces, which often offer subsidized plans for low- to middle-income earners. Second, check eligibility for Medicaid, even if your state hasn’t expanded it, as certain groups like children and pregnant women may still qualify. Lastly, consider community health centers, which provide low-cost or sliding-scale care regardless of insurance status.
Comparatively, states with lower uninsured rates often invest in outreach programs to educate residents about available options. For example, Massachusetts’ ConnectorCare program offers affordable plans for those earning up to 300% of the federal poverty level. Such initiatives demonstrate that proactive state-level efforts can significantly reduce uninsured rates. By studying these examples, other states can identify strategies to improve coverage for their populations.
In conclusion, uninsured rates by state are not merely statistical variations but reflections of policy choices and socioeconomic conditions. States with lower rates provide a roadmap for reducing coverage gaps through Medicaid expansion, subsidized plans, and targeted outreach. For those in high-uninsured states, understanding available resources and advocating for policy changes can help bridge the gap in access to healthcare.
Healthfirst: Comprehensive Medical and Dental Insurance for Your Wellbeing?
You may want to see also
Explore related products






![]()
Impact of income on coverage
Income is a decisive factor in determining whether a U.S. citizen has health insurance. Data from the U.S. Census Bureau reveals that in 2022, 8.5% of individuals in households earning below $25,000 annually were uninsured, compared to just 3.8% in households earning $75,000 or more. This disparity underscores a stark reality: lower income often equates to higher likelihood of being uninsured. The inability to afford premiums, deductibles, and copays creates a barrier to coverage, leaving millions vulnerable to financial strain from medical expenses.
Consider the mechanics of this relationship. Employer-sponsored insurance, the most common coverage type, is less accessible to low-wage workers, who are more likely to be employed in part-time, gig, or service-sector jobs that don’t offer benefits. Even when offered, these plans may consume a disproportionate share of a low-income worker’s paycheck, making them unaffordable. For example, a $200 monthly premium represents 12% of income for someone earning $20,000 annually, compared to just 3% for someone earning $80,000. This imbalance forces difficult trade-offs between health coverage and basic needs like rent or groceries.
Medicaid was designed to address this gap, providing coverage to low-income individuals and families. However, eligibility varies by state, creating a patchwork of access. In states that expanded Medicaid under the Affordable Care Act, uninsured rates among low-income adults dropped significantly—by as much as 10 percentage points in some cases. Yet, in non-expansion states, millions remain in the "coverage gap," earning too much to qualify for Medicaid but too little to afford private insurance. For instance, a single adult earning $15,000 in Texas falls into this gap, despite being just above the federal poverty level.
To mitigate these disparities, practical steps can be taken. First, policymakers could standardize Medicaid eligibility across states, ensuring consistent access regardless of geography. Second, subsidizing premiums and out-of-pocket costs for low-income individuals in the marketplace could make coverage more attainable. For individuals, exploring all available options—including community health centers, which offer sliding-scale fees—can provide temporary relief. Additionally, advocating for workplace policies that extend benefits to part-time workers could reduce the income-based coverage divide.
Ultimately, the impact of income on health insurance coverage is a symptom of broader economic inequalities. Addressing it requires systemic changes that decouple healthcare access from income level. Until then, millions will continue to face the impossible choice between financial stability and medical security, highlighting the urgent need for reform.
Medical Insurance: Customizing Your Coverage for Peace of Mind
You may want to see also
Explore related products

![Medicare and Social Security: [5 in 1] Maximize Your Retirement Benefits, Secure Medical Coverage and Quality Healthcare | Proven Strategies to Protect Your Financial Future Avoiding Costly Mistakes](https://m.media-amazon.com/images/I/61ilSrOeMoL._AC_UY218_.jpg)




![]()
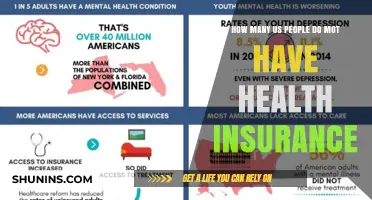
Racial disparities in insurance
According to recent data, approximately 8.5% of Americans, or around 28 million people, were uninsured in 2022. However, this figure masks significant racial disparities in insurance coverage. For instance, while 5.4% of non-Hispanic white individuals lack health insurance, the rate jumps to 9.9% for Black Americans and 19.1% for Hispanic Americans. These disparities are not merely numbers but reflect deeper systemic issues that perpetuate inequality in healthcare access.
To understand these disparities, consider the intersection of race, income, and employment. Hispanic Americans, for example, are more likely to work in low-wage jobs that do not offer employer-sponsored health insurance, a primary coverage source for most Americans. Additionally, Medicaid expansion under the Affordable Care Act (ACA) has not been adopted uniformly across states, disproportionately affecting communities of color in states that opted out. In Texas, where 18% of the population is uninsured, the decision not to expand Medicaid has left many low-income Hispanic and Black residents without affordable coverage options.
Addressing these disparities requires targeted policy interventions. One practical step is expanding Medicaid in the 10 remaining non-expansion states, which would cover an estimated 2.2 million uninsured adults, many of whom are people of color. Another strategy is increasing funding for community health centers, which serve as critical safety nets for underserved populations. For individuals, understanding eligibility for ACA subsidies or state-specific programs can help bridge coverage gaps. For example, families of four earning up to $104,800 annually may qualify for premium tax credits, yet many remain unaware of this option.
Comparatively, countries with universal healthcare systems, such as Canada or the UK, demonstrate how eliminating insurance disparities can improve health outcomes for marginalized groups. While the U.S. operates differently, adopting lessons from these models—like prioritizing equitable access over profit-driven systems—could reduce racial gaps. For instance, implementing a public option or lowering the Medicaid eligibility threshold could ensure more consistent coverage across racial lines.
Finally, advocacy plays a crucial role in dismantling these disparities. Organizations like the NAACP and the National Council of La Raza have pushed for policies addressing racial inequities in healthcare. Individuals can contribute by supporting these groups, contacting legislators, or participating in community health initiatives. By combining systemic change with grassroots efforts, the U.S. can move closer to a healthcare system where race no longer dictates access to insurance.
Illegal Immigrants: Medicare and Supplemental Insurance Access
You may want to see also
Explore related products


![]()
Effect of policy changes
Policy changes have a profound and measurable impact on the number of uninsured U.S. citizens, often acting as a lever that swings coverage rates dramatically. For instance, the Affordable Care Act (ACA) of 2010, which expanded Medicaid and established health insurance marketplaces, reduced the uninsured rate from 16% in 2010 to 8.6% in 2016. This shift highlights how legislative action can directly address gaps in coverage, particularly among low-income populations and those with pre-existing conditions. Conversely, attempts to repeal or undermine the ACA have led to fluctuations in uninsured rates, demonstrating the fragility of gains tied to specific policies.
Consider the mechanics of policy implementation: expansions of Medicaid eligibility criteria, for example, immediately increase access for millions. In states that adopted Medicaid expansion under the ACA, uninsured rates dropped by an average of 10 percentage points more than in non-expansion states. However, the effectiveness of such policies depends on state-level adoption, creating a patchwork of coverage disparities across the country. This variability underscores the importance of federal-state collaboration in policy design and execution.
A cautionary tale emerges when examining the consequences of policy reversals. The elimination of the ACA’s individual mandate penalty in 2019, for instance, contributed to a rise in uninsured rates, particularly among younger, healthier individuals who opted out of coverage. This trend illustrates the delicate balance between incentivizing enrollment and ensuring affordability. Policymakers must weigh the trade-offs: while reducing penalties may appeal to some, it risks destabilizing insurance markets and increasing the uninsured population.
Practical steps for maximizing policy impact include targeted outreach campaigns to educate underserved communities about available coverage options. For example, multilingual materials and community health workers have proven effective in reaching non-English-speaking populations. Additionally, simplifying enrollment processes—such as streamlining applications and reducing documentation requirements—can significantly boost participation rates. These measures, when paired with robust policy frameworks, create a synergistic effect that drives down uninsured numbers.
Ultimately, the effect of policy changes on uninsured rates is not just statistical but deeply human. Each percentage point represents millions of individuals gaining or losing access to essential healthcare services. Policymakers must approach reforms with a dual focus: crafting evidence-based legislation and ensuring its equitable implementation. By doing so, they can create a system where policy changes translate into tangible improvements in health coverage and outcomes for all Americans.
Top Health Insurance Providers in New Jersey: A Comprehensive Guide
You may want to see also
Explore related products



![]()
Uninsured children statistics
As of the latest data, approximately 4.3 million children in the United States lack health insurance, representing about 5.5% of all children under the age of 19. This figure, while lower than the uninsured rate for adults, still highlights a significant gap in coverage for one of the most vulnerable populations. The majority of uninsured children live in low-income families, with parents who often work in jobs that do not offer health benefits. Medicaid and the Children’s Health Insurance Program (CHIP) have been instrumental in reducing these numbers over the past two decades, but barriers such as eligibility restrictions, administrative hurdles, and lack of awareness persist.
Consider the regional disparities in uninsured children rates. Southern states, such as Texas and Florida, consistently report higher percentages of uninsured children compared to states in the Northeast and Midwest. Texas alone accounts for nearly a quarter of all uninsured children nationwide, with 1 million children lacking coverage. These disparities are often tied to state policies regarding Medicaid expansion and CHIP funding. For instance, states that have expanded Medicaid under the Affordable Care Act (ACA) tend to have lower uninsured rates among children, as eligibility thresholds are higher and more families qualify for assistance.
To address this issue, policymakers and advocates must focus on simplifying enrollment processes and increasing outreach efforts. Many eligible children remain uninsured because their parents are unaware of available programs or find the application process too complex. Schools and community organizations can play a critical role by hosting enrollment events and providing multilingual resources. Additionally, extending CHIP funding and expanding Medicaid in non-expansion states could significantly reduce the number of uninsured children. Practical steps include integrating enrollment assistance into pediatric offices and leveraging technology to streamline applications.
A comparative analysis reveals that uninsured children are more likely to forgo preventive care, such as vaccinations and well-child visits, which can lead to poorer health outcomes in the long term. For example, uninsured children are twice as likely to go without a regular source of medical care compared to their insured peers. This lack of access not only affects individual children but also places a financial burden on the healthcare system, as untreated conditions often result in costlier emergency room visits. Ensuring coverage for all children is not just a moral imperative but also an economically sound strategy.
Finally, it’s essential to recognize the long-term implications of childhood uninsurance. Children without health coverage are at higher risk of developmental delays, chronic illnesses, and reduced educational attainment. Studies show that children with consistent access to healthcare perform better in school and are more likely to graduate. By investing in programs like Medicaid and CHIP, society can break the cycle of poverty and improve outcomes for future generations. The goal should be universal coverage for children, ensuring that no child’s health—and future—is left to chance.
Medical Insurance on B1/B2 Visas: What You Need to Know
You may want to see also
Frequently asked questions
As of 2023, approximately 8% of the U.S. population, or around 27 million people, are uninsured, according to the U.S. Census Bureau.
The main reasons include high insurance costs, lack of employer-sponsored coverage, ineligibility for public programs like Medicaid, and gaps in state policies, such as not expanding Medicaid under the Affordable Care Act.
The number of uninsured individuals has fluctuated but generally increased slightly in recent years, partly due to policy changes, economic factors, and reduced enrollment in public health insurance programs.