In 2009, the average cost of health insurance for an individual in the United States varied significantly depending on factors such as location, age, and the type of plan. According to data from the Kaiser Family Foundation, the average annual premium for employer-sponsored health insurance was approximately $4,824 for single coverage and $13,375 for family coverage. For those purchasing insurance individually, costs were generally higher, with premiums averaging around $2,985 annually for single coverage. These figures highlight the financial burden of health insurance during a period marked by rising healthcare costs and economic uncertainty, setting the stage for ongoing debates about affordability and accessibility in the healthcare system.
Explore related products






What You'll Learn
- Average Monthly Premiums: Cost breakdown for individual and family health insurance plans in 2009
- Employer-Sponsored Coverage: Percentage of premiums paid by employers versus employees in 2009
- Regional Variations: Differences in health insurance costs across states and cities in 2009
- Policy Types: Comparison of HMO, PPO, and other plan costs in 2009
- Inflation Impact: How inflation affected health insurance prices from 2008 to 2009
![]()
Average Monthly Premiums: Cost breakdown for individual and family health insurance plans in 2009
In 2009, the average monthly premium for individual health insurance in the United States was approximately $215, while family plans averaged around $580. These figures, sourced from the Kaiser Family Foundation, highlight the significant financial commitment required for health coverage during that period. To understand the cost breakdown, it’s essential to examine the factors influencing these premiums, such as plan type, geographic location, and age of the insured.
Analyzing Plan Types: Individual health insurance plans in 2009 varied widely based on coverage levels. Basic plans, often with higher deductibles and limited provider networks, could cost as little as $150 per month. In contrast, comprehensive plans offering lower out-of-pocket costs and broader coverage typically ranged from $300 to $400 monthly. For family plans, the disparity was even more pronounced. A family of four might pay $450 for a high-deductible plan but upwards of $800 for a plan with extensive benefits and lower copays.
Geographic Disparities: Location played a pivotal role in determining premiums. For instance, states with higher healthcare costs, such as Massachusetts and California, saw average individual premiums of $250 to $300 per month. Meanwhile, states with lower healthcare expenses, like Alabama or Mississippi, had averages closer to $180. Family plans followed a similar pattern, with costs in high-expense states reaching $700 or more, compared to $500 in lower-cost regions.
Age and Premiums: Age was another critical factor, particularly for individual plans. Younger adults (ages 20–30) often paid premiums on the lower end of the spectrum, averaging $180–$220 per month. As individuals aged into their 40s and 50s, premiums could increase to $250–$350 due to higher perceived health risks. Family plans, however, were less age-sensitive, as they typically covered a mix of ages, with the overall cost reflecting the collective risk of all members.
Practical Tips for Cost Management: To mitigate these costs, individuals and families in 2009 could consider several strategies. First, opting for a high-deductible health plan (HDHP) paired with a Health Savings Account (HSA) could reduce monthly premiums while offering tax advantages. Second, comparing plans through employer-sponsored options or state insurance exchanges could uncover more affordable alternatives. Lastly, maintaining a healthy lifestyle and utilizing preventive care services could lower long-term healthcare expenses, indirectly reducing insurance costs.
In summary, the average monthly premiums for health insurance in 2009 reflected a complex interplay of plan type, location, and age. By understanding these factors and employing cost-saving strategies, individuals and families could navigate the financial challenges of securing adequate coverage during that time.
Top Insurance Providers Offering Medicare Supplement Plans: A Comprehensive Guide
You may want to see also
Explore related products





![]()
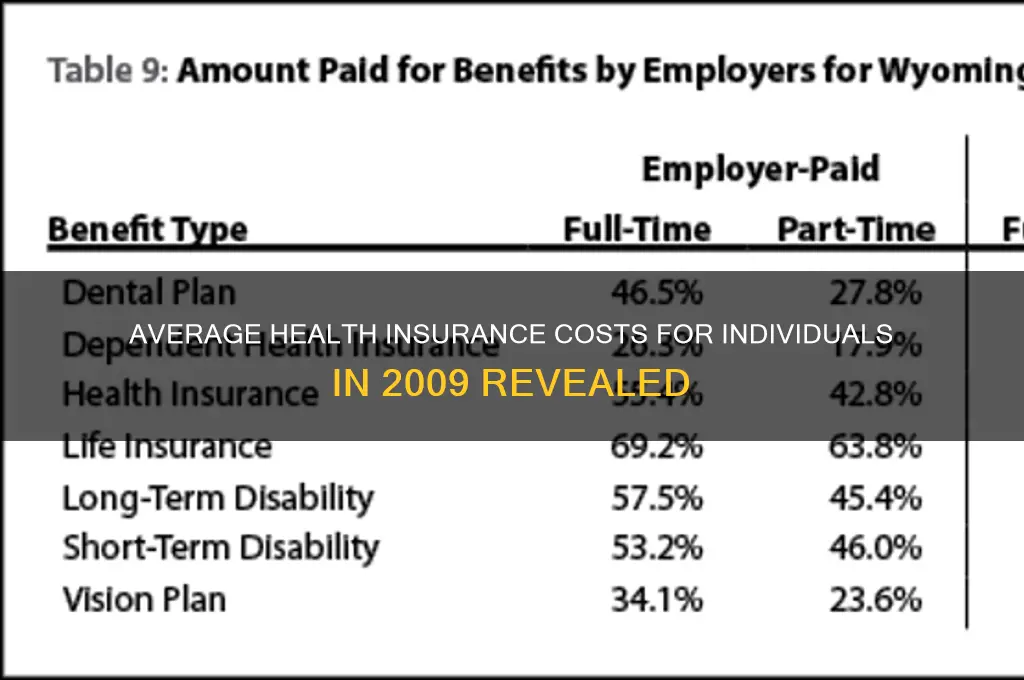
Employer-Sponsored Coverage: Percentage of premiums paid by employers versus employees in 2009
In 2009, employer-sponsored health insurance was the primary source of coverage for approximately 160 million Americans, making it a cornerstone of the nation’s healthcare system. A critical aspect of this arrangement was the division of premium costs between employers and employees. On average, employers covered about 72% of the premium for single coverage and 68% for family coverage, leaving employees to shoulder the remaining portion. This cost-sharing model reflected a long-standing tradition of employer-provided benefits, but it also highlighted growing financial pressures on workers as healthcare costs continued to rise.
To put this into perspective, consider a typical family plan in 2009, which averaged $13,375 annually. With employers covering 68%, their contribution would be roughly $9,095, while employees paid the remaining $4,280. For single coverage, the average premium was $4,824, with employers contributing approximately $3,473 and employees paying $1,351. These figures underscore the significant financial commitment required from employees, particularly for family plans, which were nearly three times more expensive than individual coverage.
However, the employer-employee split was not uniform across industries or company sizes. Larger firms, often with greater financial resources, tended to cover a higher percentage of premiums compared to small businesses. For instance, employees in small firms (3–199 workers) paid a larger share of their premiums—sometimes up to 40% for family coverage—compared to their counterparts in larger firms, where the employee contribution might be closer to 25%. This disparity often left workers in smaller companies more vulnerable to the burden of rising healthcare costs.
The implications of this cost-sharing arrangement extended beyond immediate financial strain. As premiums increased—rising 5% in 2009 alone—employees faced difficult choices, such as opting for plans with higher deductibles or forgoing coverage altogether. For example, a family earning $50,000 annually might spend nearly 10% of their pre-tax income on health insurance, leaving less room for other essentials like housing, education, or savings. This dynamic contributed to a growing debate about the sustainability of employer-sponsored coverage as the primary model for health insurance in the U.S.
In conclusion, while employer-sponsored health insurance remained a vital benefit for millions in 2009, the percentage of premiums paid by employees revealed a shifting financial burden. Understanding this split—72% for single and 68% for family coverage on average—provides insight into the challenges faced by workers, particularly those in smaller firms or lower-income brackets. As healthcare costs continued to climb, this cost-sharing model underscored the need for broader reforms to ensure affordable, accessible coverage for all.
Denied Medicare Supplemental Insurance: What's Your Next Move?
You may want to see also
Explore related products






![]()
Regional Variations: Differences in health insurance costs across states and cities in 2009
In 2009, the average cost of health insurance for an individual in the United States varied significantly depending on geographic location, with regional disparities influenced by factors such as state regulations, cost of living, and healthcare provider density. For instance, states like Massachusetts and California reported higher average premiums, often exceeding $5,000 annually for individual plans, due to their comprehensive coverage mandates and higher healthcare utilization rates. In contrast, states like Alabama and Mississippi saw lower average costs, typically below $3,500, partly because of less stringent coverage requirements and lower medical service costs.
Analyzing city-level data reveals even more pronounced differences. Urban centers like New York City and San Francisco experienced some of the highest health insurance costs in the nation, with premiums for individual plans averaging around $6,000 to $7,000 annually. These elevated costs can be attributed to higher provider fees, greater demand for specialized care, and the overall higher cost of living. Conversely, smaller cities in the Midwest and South, such as Indianapolis or Birmingham, reported significantly lower averages, often in the range of $2,500 to $3,500, reflecting lower healthcare expenses and less competitive insurance markets.
To navigate these regional variations, individuals should consider their location-specific factors when selecting a health insurance plan. For example, residents in high-cost areas might prioritize plans with broader provider networks to ensure access to affordable care, while those in lower-cost regions could opt for high-deductible plans to reduce premiums. Additionally, understanding state-specific mandates, such as coverage for pre-existing conditions or preventive services, can help consumers make informed decisions tailored to their regional context.
A comparative analysis of regional trends in 2009 highlights the impact of policy decisions on insurance costs. States with robust public health programs, like Massachusetts, often had higher premiums but lower out-of-pocket expenses, whereas states with fewer regulations saw lower premiums but higher individual costs for services. This underscores the importance of balancing affordability with access to care, a challenge that persists in today’s healthcare landscape. By examining these 2009 variations, individuals can better anticipate how regional factors might affect their current insurance choices.
Finally, practical tips for managing regional cost differences include leveraging employer-sponsored plans, which often mitigate geographic price disparities, and exploring state-run health insurance marketplaces for subsidized options. For those in high-cost areas, health savings accounts (HSAs) paired with high-deductible plans can provide tax advantages and cost control. Understanding these regional nuances empowers consumers to optimize their health insurance decisions, ensuring both affordability and adequate coverage in their specific location.
Life Insurance Options for Genetic Hypertrophic Cardiomyopathy Patients
You may want to see also
Explore related products






![]()
Policy Types: Comparison of HMO, PPO, and other plan costs in 2009
In 2009, the average annual premium for employer-sponsored health insurance was $5,049 for single coverage and $13,375 for family coverage, according to the Kaiser Family Foundation. These figures, however, mask significant variations based on the type of health insurance plan. Among the most common were Health Maintenance Organizations (HMOs), Preferred Provider Organizations (PPOs), and other plans like Point of Service (POS) and Exclusive Provider Organizations (EPOs). Each plan type offered distinct cost structures, influenced by factors such as flexibility, provider networks, and out-of-pocket expenses.
HMOs, known for their cost-effectiveness, typically featured lower premiums in 2009 compared to PPOs. This was largely due to their restrictive network of providers and requirement for a primary care physician (PCP) to coordinate care. For instance, an HMO plan might have had an average monthly premium of $250 for an individual, with a modest deductible of $500. However, enrollees faced higher costs if they sought care outside the network, which was often not covered at all. This made HMOs ideal for those who prioritized affordability and were willing to accept limited provider choices.
PPOs, on the other hand, offered greater flexibility but at a higher cost. In 2009, the average monthly premium for a PPO plan could be around $350 for an individual, with a deductible of $1,000 or more. PPOs allowed members to see out-of-network providers, though at a significantly higher cost. This flexibility was particularly appealing to individuals who preferred access to a broader range of specialists or had established relationships with specific doctors. However, the trade-off was higher premiums and out-of-pocket costs, making PPOs less budget-friendly than HMOs.
Other plan types, such as POS and EPOs, occupied a middle ground in terms of cost and flexibility. A POS plan, for example, combined elements of HMOs and PPOs, requiring a PCP while allowing out-of-network care at an additional cost. In 2009, a POS plan might have had a monthly premium of $300, with a deductible of $750. EPOs, which offered a network of providers but no out-of-network coverage, were slightly cheaper than PPOs but more expensive than HMOs. These plans were suitable for individuals seeking a balance between cost and flexibility.
When comparing these plan types in 2009, it’s clear that the choice depended on individual needs and financial circumstances. For those on a tight budget, HMOs provided the most affordable option, despite their limitations. PPOs, while more expensive, offered unparalleled flexibility for those who valued choice and access. POS and EPOs served as viable alternatives for those seeking a middle ground. Understanding these differences allowed consumers to make informed decisions, ensuring their health insurance aligned with both their medical needs and financial capabilities.
Who Insured First American Title Company: Uncovering the Early Backers
You may want to see also
Explore related products






![]()
Inflation Impact: How inflation affected health insurance prices from 2008 to 2009
Between 2008 and 2009, the average cost of health insurance for an individual in the United States rose by approximately 5.5%, outpacing the general inflation rate of 0.4% during the same period. This disparity highlights how inflation, combined with other economic factors, disproportionately affected healthcare costs. For context, while the Consumer Price Index (CPI) remained relatively stable, medical care costs increased by 3.4% in 2009 alone, according to the Bureau of Labor Statistics. This trend underscores the unique sensitivity of health insurance to inflationary pressures, as providers often pass rising operational costs onto consumers.
To understand this impact, consider the mechanics of inflation in the healthcare sector. Inflation typically drives up wages, administrative expenses, and the cost of medical supplies and technology. For instance, the price of prescription drugs, a significant component of health insurance claims, rose by 5.4% in 2009, according to the Kaiser Family Foundation. Insurers, facing these increased costs, adjusted premiums to maintain profitability. A family of four, for example, saw their average annual health insurance premium climb from $12,680 in 2008 to $13,375 in 2009—a $695 increase that far exceeded general inflation.
However, inflation alone does not fully explain the rise in health insurance costs. The 2008 financial crisis led to higher unemployment rates, reducing the number of employer-sponsored insurance plans and pushing more individuals into the individual market, where premiums are typically higher. This shift increased demand for individual policies, giving insurers leverage to raise prices. Additionally, the anticipation of healthcare reform in 2009 created uncertainty, prompting some insurers to preemptively increase premiums to hedge against potential regulatory changes.
Practical implications of this inflationary impact are evident in consumer behavior. For those aged 55–64, a demographic already facing higher premiums due to age-related risks, the 2008–2009 increase meant an average premium rise of 8%, according to AARP data. To mitigate costs, many individuals opted for high-deductible plans, which reduced monthly premiums but increased out-of-pocket expenses. For example, a 40-year-old in 2009 might have chosen a plan with a $2,500 deductible to save $100–$200 monthly, a trade-off that became more common as inflation squeezed household budgets.
In conclusion, while inflation played a significant role in driving up health insurance costs from 2008 to 2009, it was compounded by economic fallout from the financial crisis and industry-specific factors. This period serves as a case study in how macroeconomic trends intersect with sector-specific dynamics to shape consumer expenses. For individuals, understanding these interactions is crucial for making informed decisions, such as selecting plans with lower premiums but higher deductibles or exploring subsidies and assistance programs to offset rising costs.
Who is Sam's Club's Insurance Company? A Comprehensive Guide
You may want to see also
Frequently asked questions
In 2009, the average annual premium for employer-sponsored health insurance was approximately $5,049 for single coverage and $13,375 for family coverage, according to the Kaiser Family Foundation.
Yes, health insurance premiums continued to rise in 2009. Premiums for employer-sponsored insurance increased by about 5.5% for single coverage and 5.8% for family coverage compared to 2008.
In 2009, the average worker’s contribution to health insurance premiums accounted for about 8.8% of their income for single coverage and 20.7% for family coverage, based on median household income data.
Yes, individual health insurance plans were generally more expensive than employer-sponsored plans in 2009. Individual plans often lacked the group purchasing power and subsidies that employer plans provided.
Health insurance costs in 2009 varied significantly by state due to differences in healthcare regulations, provider costs, and market competition. For example, states like Massachusetts and California had higher premiums compared to states like Alabama or Idaho.































