The U.S. health insurance system often excludes abortion coverage due to a complex interplay of federal and state laws, political ideologies, and private insurer policies. The Hyde Amendment, enacted in 1976, prohibits the use of federal funds for abortion services except in cases of rape, incest, or life endangerment, significantly limiting Medicaid coverage for millions of low-income individuals. Additionally, many private insurance plans, particularly those offered through employer-sponsored programs, exclude abortion coverage, either due to state-level restrictions or to avoid controversy. Even in states with more progressive policies, access remains uneven, as insurers may opt out of covering abortion services. These exclusions disproportionately affect marginalized communities, particularly women of color and those with limited financial resources, exacerbating existing healthcare disparities and restricting reproductive autonomy.
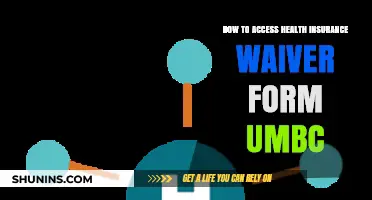
| Characteristics | Values |
|---|---|
| Hyde Amendment | Prohibits federal funding (e.g., Medicaid) from covering abortions except in cases of rape, incest, or life endangerment. |
| State-Level Restrictions | 26 states restrict abortion coverage in state-regulated insurance plans, even for private plans. |
| Private Insurance Coverage | Only 12% of employer-sponsored plans cover abortion without restrictions as of 2023. |
| Medicaid Coverage | Only 16 states use their own funds to cover abortions for Medicaid enrollees beyond Hyde restrictions. |
| Affordable Care Act (ACA) Plans | ACA plans can cover abortion, but 26 states ban abortion coverage in ACA marketplace plans. |
| Out-of-Pocket Costs | Average out-of-pocket cost for abortion is $500-$1,000, with limited financial assistance available. |
| Provider Availability | 58% of U.S. counties have no abortion providers, limiting access even with insurance. |
| Waiting Periods and Counseling | 38 states require counseling or waiting periods, increasing costs and barriers to insurance coverage. |
| Insurance Opt-Outs | Employers in 20 states can opt out of providing abortion coverage in health plans due to moral or religious objections. |
| Post-Dobbs Landscape | After Dobbs v. Jackson Women’s Health Organization, 14 states banned abortion entirely, further limiting insurance coverage. |
Explore related products






What You'll Learn
- State-Level Restrictions: Many states limit abortion coverage in health plans, even for private insurers
- Hyde Amendment: Bans federal funding for abortions, excluding Medicaid and other programs
- Employer-Based Plans: Many employers opt out of abortion coverage in health insurance offerings
- Marketplace Plan Limitations: Affordable Care Act plans often exclude abortion coverage in many states
- Conscience Clauses: Allow insurers and providers to refuse abortion coverage based on moral grounds
![]()
State-Level Restrictions: Many states limit abortion coverage in health plans, even for private insurers
In the United States, state-level restrictions on abortion coverage in health insurance plans have created a patchwork of access disparities, often leaving individuals at the mercy of their geographic location. Consider this: as of 2023, 26 states have enacted laws prohibiting the use of state funds for abortion coverage, even in cases of rape, incest, or life-threatening conditions. This doesn’t just affect public insurance programs like Medicaid; it extends to private insurers operating within those states. For instance, in Texas, private health plans are barred from including abortion coverage unless the procedure is necessary to save the life of the mother. Such restrictions force individuals to pay out-of-pocket for abortion services, which can range from $500 to $3,000 depending on the stage of pregnancy and location, effectively pricing many out of access.
Analyzing the impact of these restrictions reveals a systemic bias against low-income individuals and marginalized communities. States with the most stringent abortion coverage bans often have higher rates of uninsured populations, exacerbating existing health inequities. For example, in Mississippi, where abortion coverage is severely restricted, nearly 13% of residents lack health insurance, compared to the national average of 8.6%. Private insurers in these states are legally bound to comply with state mandates, leaving them unable to offer comprehensive reproductive health coverage even if they wish to. This creates a paradox: while private insurance is meant to provide broader benefits, state laws effectively narrow its scope, undermining the very purpose of private coverage.
To navigate these restrictions, individuals must take proactive steps. First, carefully review your health insurance policy to understand what is and isn’t covered. Look for terms like “maternity care” or “pregnancy-related services” and cross-reference them with state laws. Second, consider supplemental insurance plans or abortion funds, which can help offset out-of-pocket costs. Organizations like the National Network of Abortion Funds provide financial assistance and resources for those in need. Third, if you’re considering relocating or changing jobs, research state laws and employer policies on abortion coverage—some companies, particularly those with a national presence, may offer more inclusive benefits regardless of state restrictions.
A comparative look at states with and without these restrictions highlights the stark differences in access. In California, private insurers are required by law to cover abortion services as part of basic health care, ensuring that cost is not a barrier. Conversely, in Idaho, private plans are prohibited from including abortion coverage unless the pregnancy threatens the life of the mother. This contrast underscores how state-level policies directly shape reproductive rights, often overriding individual choice and medical necessity. The takeaway is clear: state restrictions on abortion coverage in private insurance plans are not just legal technicalities—they are deliberate barriers that limit access to essential health care.
Finally, understanding the broader implications of these restrictions is crucial. By limiting abortion coverage, states not only infringe on reproductive autonomy but also contribute to long-term economic and health consequences. Unintended pregnancies can lead to increased reliance on public assistance programs, higher maternal mortality rates, and delayed educational and career opportunities. Advocating for policy changes at the state level, such as repealing coverage bans and mandating comprehensive reproductive health care, is essential. Until then, individuals must remain informed, resourceful, and proactive in securing the care they need, despite the systemic obstacles in place.
Medicare and Insurance: What's the Difference?
You may want to see also
Explore related products






![]()
Hyde Amendment: Bans federal funding for abortions, excluding Medicaid and other programs
The Hyde Amendment, first enacted in 1976, prohibits the use of federal funds to pay for abortion services, with narrow exceptions. This restriction primarily affects individuals who rely on Medicaid, the federal-state program that provides health coverage to low-income individuals. While the amendment excludes cases of rape, incest, or life endangerment, its broad application has created significant barriers to abortion access for millions of Americans. For context, nearly 1 in 5 women of reproductive age are enrolled in Medicaid, making this policy a critical determinant of who can afford abortion care.
Consider the practical implications: a 25-year-old Medicaid recipient in Texas, earning $15,000 annually, would need to cover the full cost of an abortion procedure, averaging $500–$1,000 for the first trimester. Without federal funding, this expense often forces individuals to delay care, seek unsafe alternatives, or forgo the procedure altogether. The Hyde Amendment effectively penalizes low-income individuals, disproportionately impacting women of color, who are more likely to rely on Medicaid. This financial burden underscores how systemic policies intersect with socioeconomic disparities to restrict reproductive autonomy.
Critics argue that the Hyde Amendment violates the principle of equitable healthcare by treating abortion as a separate, non-essential service. Unlike prenatal care, delivery, or even sterilization procedures, abortion is singled out for exclusion from federal funding. This distinction ignores the reality that abortion is a time-sensitive medical intervention, often necessary for physical or mental health. For instance, a study in the *American Journal of Public Health* found that women denied abortions were more likely to experience long-term economic hardship compared to those who received the procedure.
To navigate this landscape, advocates recommend several strategies. First, individuals should verify their insurance coverage by contacting their provider directly, as state-level policies may offer additional protections. Second, organizations like the National Network of Abortion Funds provide financial assistance to those unable to afford out-of-pocket costs. Lastly, supporting legislative efforts to repeal the Hyde Amendment remains crucial. The EACH Woman Act, for example, seeks to ensure coverage for abortion care under federal programs, though it has yet to pass Congress.
In conclusion, the Hyde Amendment exemplifies how the U.S. health insurance system systematically excludes abortion care, particularly for marginalized populations. Its impact extends beyond policy, shaping the lived experiences of millions who face financial and logistical barriers to accessing essential healthcare. Addressing this inequity requires both immediate practical solutions and long-term advocacy for systemic change.
Medical Insurance: Choosing the Right Plan for You
You may want to see also
Explore related products






![]()
Employer-Based Plans: Many employers opt out of abortion coverage in health insurance offerings
Employer-based health insurance plans cover approximately 157 million Americans, yet many of these plans explicitly exclude abortion coverage. This exclusion is often rooted in a combination of legal restrictions, corporate policies, and religious or moral objections. For instance, the Hyde Amendment, which prohibits federal funding for abortions except in cases of rape, incest, or life endangerment, influences employer decisions by setting a precedent for limiting coverage. As a result, employees seeking abortion services frequently face out-of-pocket costs ranging from $500 to $2,000, depending on the procedure and location.
Consider the practical implications for workers, particularly those in low-wage jobs. A 2020 study found that 60% of abortion patients are already parents, and many struggle to afford both the procedure and associated travel or childcare costs. When employer-based plans exclude abortion coverage, these individuals are forced to choose between financial stability and accessing necessary healthcare. This disparity disproportionately affects women of color and those in states with restrictive abortion laws, exacerbating existing healthcare inequities.
Employers often justify opting out of abortion coverage by citing cost concerns or a desire to remain neutral on controversial issues. However, this neutrality argument falls short when examined critically. By excluding abortion coverage, employers effectively take a stance that limits reproductive autonomy. Furthermore, the cost argument is undermined by the fact that covering abortion is cost-effective in the long term, as it prevents more expensive complications from unsafe procedures or unwanted pregnancies.
To address this gap, employees can advocate for change by organizing within their workplaces. Steps include forming coalitions with coworkers, drafting petitions, and engaging in open dialogue with HR departments. Practical tips for advocacy include highlighting the legal and ethical obligations of employers to provide comprehensive healthcare and citing data on the financial and health benefits of inclusive coverage. Additionally, employees can leverage state-specific laws, such as those in California and New York, which mandate abortion coverage in employer-based plans, as examples of feasible policy changes.
In conclusion, the exclusion of abortion coverage in employer-based plans is a systemic issue with far-reaching consequences. By understanding the legal, financial, and ethical dimensions of this practice, employees and advocates can push for more equitable healthcare policies. This requires not only awareness but also strategic action to challenge the status quo and ensure reproductive rights are integrated into workplace benefits.
Insurance Companies' Profit Strategies in Medicaid Explained
You may want to see also
Explore related products






![]()
Marketplace Plan Limitations: Affordable Care Act plans often exclude abortion coverage in many states
The Affordable Care Act (ACA) marketplace plans, designed to expand healthcare access, often fall short when it comes to abortion coverage. In states with restrictive policies, these plans frequently exclude abortion services, leaving individuals to navigate a complex and costly landscape. This limitation is not merely a policy detail but a significant barrier to reproductive healthcare, particularly for low-income individuals and those in conservative states. Understanding these restrictions is crucial for anyone seeking comprehensive coverage.
Consider the mechanics of ACA plans and abortion coverage. While the ACA does not explicitly prohibit abortion coverage, it allows states to decide whether marketplace plans can include it. As of 2023, 26 states restrict abortion coverage in ACA plans, often limiting it to cases of rape, incest, or life endangerment. This patchwork of regulations means that a woman’s access to abortion coverage depends largely on her zip code. For example, in Texas, marketplace plans cannot cover abortion unless the pregnancy threatens the mother’s life, while in California, most plans include comprehensive abortion coverage. This disparity highlights the fragmented nature of reproductive healthcare in the U.S.
For those in restrictive states, the financial burden of abortion can be overwhelming. The average cost of a first-trimester abortion ranges from $500 to $1,000, a significant expense for individuals without coverage. While some may turn to Medicaid, federal law (the Hyde Amendment) prohibits federal funding for abortion except in limited circumstances, further narrowing options. Private insurance outside the marketplace might offer coverage, but these plans are often more expensive and out of reach for many. Practical steps for individuals include researching state-specific policies, exploring standalone abortion coverage riders (where available), and seeking financial assistance through organizations like the National Abortion Federation.
The exclusion of abortion coverage in ACA plans also raises ethical and health equity concerns. Denying coverage disproportionately affects marginalized communities, including women of color and those with lower incomes, who are less likely to afford out-of-pocket costs. This exclusion perpetuates systemic inequalities, as those with means can access private insurance or pay out of pocket, while others face insurmountable barriers. Advocates argue that reproductive healthcare, including abortion, should be treated as essential health coverage, not a political bargaining chip.
In conclusion, the limitations of ACA marketplace plans on abortion coverage underscore the broader challenges of the U.S. healthcare system. While the ACA has expanded access to insurance, its reliance on state-level decisions has created a system where reproductive rights are unevenly protected. For individuals, understanding these limitations is the first step toward advocating for change and navigating available resources. Policymakers, meanwhile, must address these gaps to ensure that healthcare coverage is truly comprehensive and equitable.
Medicaid Health Insurance: Choosing the Right Plan for You
You may want to see also
Explore related products






![]()
Conscience Clauses: Allow insurers and providers to refuse abortion coverage based on moral grounds
Conscience clauses embedded in U.S. health insurance policies grant insurers and providers the legal right to deny abortion coverage based on personal, religious, or moral objections. These clauses, often framed as protections for individual beliefs, create systemic barriers to care by prioritizing the values of corporations or healthcare professionals over the medical needs of patients. For instance, in states like Texas and Missouri, insurers have invoked conscience clauses to exclude abortion services entirely from their plans, even in cases of ectopic pregnancies or fetal anomalies, where delaying care can lead to severe health risks.
The practical impact of these clauses extends beyond the procedure itself. Patients seeking abortion care often face unexpected out-of-pocket costs, ranging from $500 to $2,000, depending on gestational age and location. For low-income individuals, this financial burden can be insurmountable, forcing them to delay or forgo care altogether. A 2021 study by the Guttmacher Institute found that 75% of abortion patients already face logistical challenges, such as travel and childcare, and the added cost of uninsured procedures exacerbates these hardships. Conscience clauses, therefore, do not merely reflect moral disagreements—they actively contribute to health disparities.
From a legal standpoint, conscience clauses operate within a framework established by laws like the Weldon Amendment, which prohibits federal funding for entities that discriminate against providers refusing to participate in abortions. While intended to protect individual providers, this legislation has been interpreted broadly to shield insurers and employers who exclude abortion coverage. For example, in 2022, a federal court upheld an insurer’s decision to deny coverage for a medication abortion, citing the Weldon Amendment as justification. This interpretation highlights how conscience clauses are weaponized to restrict access under the guise of religious freedom.
To navigate this landscape, patients must proactively scrutinize their insurance plans for abortion exclusions. Tools like the National Women’s Law Center’s "Cover Abortion" database can help identify plans with coverage gaps. Advocacy groups also recommend contacting insurers directly to confirm policy details, as exclusions are often buried in fine print. For those without coverage, organizations like the National Abortion Federation offer financial assistance, though demand frequently outstrips available funds. Ultimately, conscience clauses underscore the need for legislative reforms that prioritize medical necessity over moral objections.
Annual Health Insurance Switching Trends: How Many People Change Plans?
You may want to see also
Frequently asked questions
Coverage for abortion services varies widely in the US. Many private insurance plans exclude abortion coverage, and federal programs like Medicaid are restricted by the Hyde Amendment, which prohibits federal funding for abortions except in cases of rape, incest, or life endangerment.
State laws significantly influence abortion coverage. Some states mandate that private insurance plans cover abortion, while others explicitly ban such coverage. Additionally, states can impose restrictions on Medicaid coverage beyond federal requirements, further limiting access.
Yes, exceptions exist but are limited. Federal law requires coverage in cases of rape, incest, or life endangerment for certain plans. Some states or employers may offer broader coverage, but these are exceptions rather than the norm.