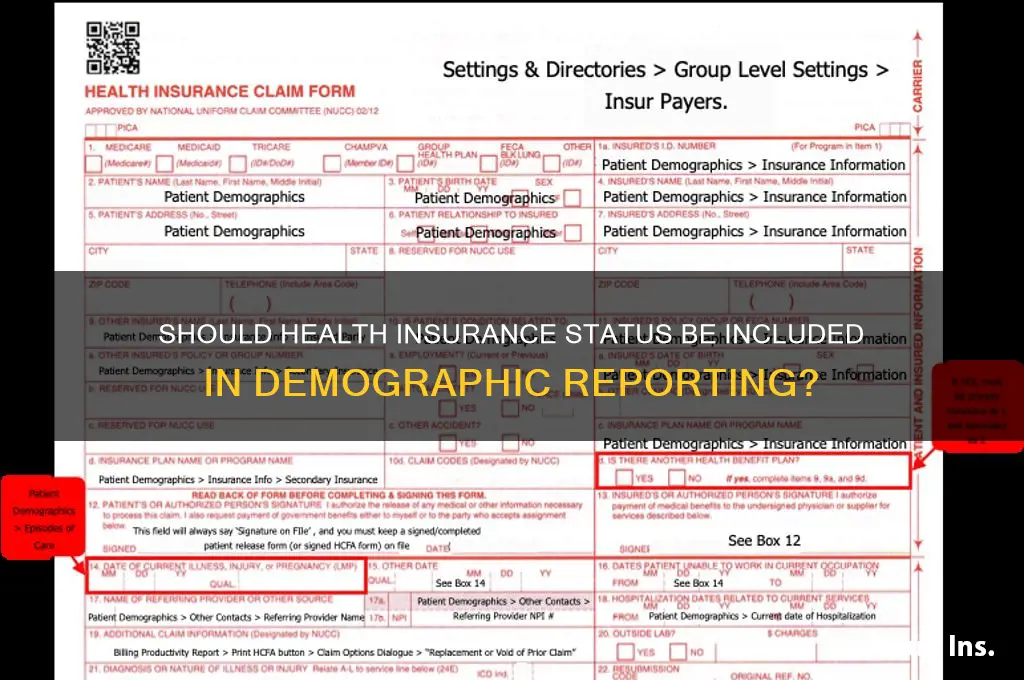
The question of whether to report health insurance status in demographics is a critical one, as it intersects with issues of healthcare access, socioeconomic disparities, and data privacy. Including insurance status in demographic data can provide valuable insights into population health, identify gaps in coverage, and inform policy interventions aimed at reducing inequities. However, it also raises concerns about stigmatization, potential misuse of sensitive information, and the ethical implications of linking insurance status to other demographic factors. Balancing the benefits of enhanced data utility with the need to protect individual privacy and avoid reinforcing biases is essential in determining whether and how health insurance status should be reported in demographic analyses.
| Characteristics | Values |
|---|---|
| Relevance to Healthcare Access | Strong indicator of access to healthcare services and preventive care. |
| Impact on Health Outcomes | Uninsured individuals often face worse health outcomes and delayed care. |
| Socioeconomic Indicator | Closely tied to income, education, and employment status. |
| Policy and Research Utility | Essential for policy-making, resource allocation, and health disparities research. |
| Ethical Considerations | Potential for stigmatization or discrimination based on insurance status. |
| Data Privacy Concerns | Sensitive information requiring strict confidentiality measures. |
| Standardization Challenges | Variations in insurance types (e.g., private, public, uninsured) complicate reporting. |
| Legal and Regulatory Requirements | Some jurisdictions mandate reporting of insurance status for specific studies. |
| Survey and Data Collection Burden | Adds complexity to demographic surveys but provides critical insights. |
| Global Applicability | Relevance varies by country based on healthcare system structure. |
| Latest Trends | Increasing emphasis on insurance status in demographic reporting for equity analysis. |
Explore related products






What You'll Learn
- Ethical implications of reporting health insurance status in demographic data collection
- Impact on healthcare access and disparities based on insurance reporting
- Privacy concerns and data protection in insurance status disclosure
- Role of insurance status in health research and policy-making
- Potential biases in studies due to incomplete insurance status reporting
![]()
Ethical implications of reporting health insurance status in demographic data collection
Reporting health insurance status in demographic data collection raises critical ethical concerns, particularly around privacy, equity, and potential misuse. Health insurance status is a sensitive indicator tied to socioeconomic factors, employment, and access to care. Including it in demographic data could inadvertently expose individuals to discrimination, such as in employment or housing, where uninsured or underinsured status might be misinterpreted as a marker of financial instability. For instance, a study by the *Journal of Health Economics* found that uninsured individuals are often perceived as less employable, even when controlling for other factors. This underscores the need for strict safeguards if such data is collected.
From an analytical perspective, the inclusion of health insurance status can skew research outcomes if not handled carefully. Researchers might conflate insurance status with health outcomes, overlooking systemic barriers to care. For example, a dataset showing higher mortality rates among the uninsured might suggest personal responsibility rather than systemic failures in healthcare access. This misinterpretation could lead to policy recommendations that exacerbate disparities rather than address root causes. Thus, while the data can be valuable, its collection and analysis require nuanced methodologies to avoid reinforcing biases.
A persuasive argument against routine reporting of health insurance status lies in its potential to stigmatize vulnerable populations. Low-income individuals, undocumented immigrants, and gig workers are disproportionately uninsured, and their representation in datasets could amplify existing marginalization. For instance, a 2020 survey by the Kaiser Family Foundation revealed that 45% of uninsured adults avoided seeking care due to cost concerns. Highlighting their insurance status in demographic data might further discourage them from engaging with healthcare systems, creating a cycle of avoidance and poorer health outcomes.
Comparatively, countries with universal healthcare systems rarely collect insurance status in demographic data, as it is irrelevant to access. In contrast, the U.S. system’s reliance on employer-based insurance makes this data point more salient but also more fraught. A practical tip for organizations considering this collection is to adopt a tiered approach: collect insurance status only when directly relevant to the study (e.g., healthcare access research) and ensure robust anonymization and consent protocols. For example, using broad categories like “insured,” “uninsured,” and “prefer not to disclose” can reduce identifiability while retaining analytical utility.
In conclusion, while reporting health insurance status in demographic data can provide valuable insights, it demands careful ethical consideration. Organizations must weigh the benefits against risks of discrimination, misinterpretation, and stigmatization. Implementing strict data protection measures, limiting collection to specific contexts, and prioritizing participant consent are essential steps to mitigate these risks. As with any sensitive data, the guiding principle should be “do no harm”—ensuring that the pursuit of knowledge does not come at the expense of individual dignity or equity.
Starting a Medicare Insurance Agency: Steps to Success
You may want to see also
Explore related products






![]()
Impact on healthcare access and disparities based on insurance reporting
Reporting health insurance status in demographics can either illuminate or exacerbate healthcare disparities, depending on how the data is used. When insurance status is systematically tracked, it becomes possible to identify populations with higher rates of uninsurance or underinsurance. For instance, data from the U.S. Census Bureau consistently shows that Hispanic and Black individuals are more likely to be uninsured compared to their White counterparts. This granular insight allows policymakers to target interventions, such as expanding Medicaid eligibility or funding community health centers in underserved areas. Without this data, disparities remain invisible, and resources may be misallocated, perpetuating inequities.
However, the act of reporting insurance status is not without risks. It can inadvertently stigmatize uninsured individuals, leading to implicit bias in healthcare delivery. A 2018 study published in *Health Affairs* found that providers were less likely to recommend preventive services to uninsured patients, assuming they lacked the means to follow through. This highlights a critical caution: collecting insurance data must be paired with training to ensure it does not influence clinical decision-making negatively. The goal should be to use this information as a tool for advocacy, not as a barrier to care.
From a practical standpoint, integrating insurance status into demographic reporting requires careful design. For example, electronic health records (EHRs) could prompt providers to ask about insurance during intake but also flag patients for financial counseling or assistance programs. Hospitals in states like California have successfully implemented such systems, reducing out-of-pocket costs for low-income patients by 30%. This approach turns data collection into a proactive step toward equity, rather than a passive observation of inequality.
Ultimately, the impact of reporting insurance status hinges on intent and implementation. If used to identify gaps and drive policy change, it can be a powerful force for reducing disparities. But if mishandled, it risks becoming another layer of systemic bias. The takeaway is clear: insurance reporting should be mandatory but must be coupled with safeguards to ensure it serves as a bridge to care, not a barrier.
Understanding Insurance Coverage for One Medical Services
You may want to see also
Explore related products

$163.1 $245.95

$13.87 $29.99




![]()
Privacy concerns and data protection in insurance status disclosure
Health insurance status, when disclosed in demographic data, can serve as a double-edged sword. On one hand, it provides valuable insights for policymakers, researchers, and healthcare providers to identify gaps in coverage and allocate resources effectively. On the other hand, it raises significant privacy concerns, as this information is highly sensitive and can be misused if not protected adequately. The challenge lies in balancing the utility of such data with the individual’s right to privacy, a delicate task that requires robust data protection measures.
Consider the potential risks: unauthorized access to insurance status data could lead to discrimination in employment, housing, or even social relationships. For instance, an employer might hesitate to hire someone with a pre-existing condition if their insurance status suggests higher healthcare costs. Similarly, landlords or lenders might use this information to make biased decisions. These scenarios underscore the need for stringent data protection laws and ethical guidelines governing the collection and use of such data. The Health Insurance Portability and Accountability Act (HIPAA) in the U.S. is a prime example of legislation designed to safeguard health information, but its application to demographic reporting remains a gray area.
To mitigate these risks, organizations collecting demographic data must adopt a multi-layered approach to data protection. Encryption, anonymization, and access controls are essential tools. For example, data should be stored in encrypted formats, and personally identifiable information (PII) should be removed or masked whenever possible. Access to such data should be restricted to authorized personnel only, with regular audits to ensure compliance. Additionally, individuals should be informed about how their data will be used and given the option to opt out if they feel uncomfortable disclosing their insurance status.
A comparative analysis of global practices reveals varying approaches to this issue. In countries like Canada and the UK, where healthcare is publicly funded, insurance status is less of a concern, as coverage is universal. However, in the U.S., where private insurance dominates, the stakes are higher. European nations, guided by the General Data Protection Regulation (GDPR), impose strict limits on the collection and processing of health-related data, offering a model for other regions to follow. By studying these examples, we can identify best practices that prioritize both data utility and individual privacy.
Ultimately, the decision to report health insurance status in demographics should not be taken lightly. While the data can drive meaningful improvements in healthcare policy and delivery, the potential for misuse demands careful consideration. Organizations must weigh the benefits against the risks, implement robust data protection measures, and ensure transparency with individuals whose data is being collected. Striking this balance is not just a legal obligation but a moral imperative to protect the dignity and rights of every individual.
Does Health Insurance Cover Probiotics? What You Need to Know
You may want to see also
Explore related products





![]()
Role of insurance status in health research and policy-making
Health insurance status is a critical determinant of healthcare access, utilization, and outcomes, yet its inclusion in demographic reporting remains inconsistent across research and policy frameworks. This variability raises questions about the role of insurance status in shaping health disparities and informing interventions. For instance, studies show that uninsured individuals are 25% less likely to receive preventive care, such as cancer screenings, compared to their insured counterparts. This gap underscores the need to systematically report insurance status to identify at-risk populations and tailor public health strategies effectively.
In health research, insurance status serves as a proxy for socioeconomic factors that influence health behaviors and outcomes. Researchers must account for insurance coverage to avoid confounding variables when analyzing disparities. For example, a study on diabetes management might find that uninsured patients have higher HbA1c levels, but without controlling for insurance status, the results could be misinterpreted as purely biological rather than systemic failures. Reporting insurance status ensures that findings are actionable, enabling policymakers to address root causes rather than symptoms.
Policy-making relies on accurate demographic data to allocate resources and design targeted interventions. Including insurance status in demographic reports allows policymakers to identify coverage gaps and their downstream effects. For instance, Medicaid expansion under the Affordable Care Act reduced uninsured rates by 40% in participating states, leading to improved health outcomes for low-income adults. By reporting insurance status, policymakers can track the impact of such initiatives and advocate for evidence-based reforms. Omitting this data risks perpetuating inequities by overlooking systemic barriers to care.
However, reporting insurance status is not without challenges. It requires standardized data collection methods to ensure comparability across studies and regions. Researchers and policymakers must also consider the dynamic nature of insurance coverage, as individuals may transition between insured and uninsured statuses over time. Longitudinal studies, such as those tracking insurance changes annually, provide a more nuanced understanding of how coverage fluctuations affect health trajectories. Practical tips include using validated survey instruments and linking administrative data to enhance accuracy.
In conclusion, the role of insurance status in health research and policy-making is indispensable for addressing health disparities and informing equitable interventions. By systematically reporting this demographic, stakeholders can uncover patterns, evaluate policies, and advocate for systemic change. While challenges exist, the benefits of including insurance status far outweigh the costs, making it a critical component of comprehensive health data frameworks.
Night Guards: Are They Covered by Medical Insurance?
You may want to see also
Explore related products






![]()
Potential biases in studies due to incomplete insurance status reporting
Incomplete insurance status reporting in demographic data introduces selection bias, skewing study populations toward individuals with stable coverage. This oversight disproportionately excludes vulnerable groups—low-income, minority, or gig-economy workers—who are more likely to be uninsured or underinsured. For instance, a study on chronic disease management might overrepresent patients with consistent access to care, masking disparities in health outcomes for those without insurance. Researchers must acknowledge this bias, as it undermines generalizability and perpetuates systemic inequalities in healthcare research.
Consider the analytical challenge: without insurance status, studies cannot control for confounding variables like healthcare access or preventive care utilization. A trial evaluating medication adherence might attribute non-compliance to patient behavior, ignoring the financial barriers uninsured participants face. To mitigate this, researchers should stratify data by insurance status or employ sensitivity analyses to estimate its impact. Tools like multiple imputation for missing data can also help, but transparency about limitations remains critical for interpreting results.
From a practical standpoint, failing to report insurance status hampers policy-making and resource allocation. For example, a study on emergency department overuse might conclude that patient education is the solution, while uninsured individuals may lack alternatives for primary care. Policymakers need granular data to design interventions—such as expanding Medicaid or subsidizing premiums—that address root causes. Researchers must prioritize collecting and reporting insurance data to ensure their findings inform equitable solutions.
Finally, the ethical imperative cannot be ignored. Incomplete insurance reporting risks stigmatizing uninsured populations by attributing health disparities solely to individual behaviors. A study on diabetes outcomes, for instance, might blame poor glycemic control on non-adherence without considering the cost of insulin or specialist visits. By explicitly documenting insurance status, researchers can highlight structural barriers and advocate for systemic changes, aligning their work with principles of social justice and health equity.
Accident Insurance: Protecting Employees from Financial Risk
You may want to see also
Frequently asked questions
Yes, including health insurance status in demographic data provides valuable insights into access to healthcare, socioeconomic disparities, and potential barriers to treatment, aiding in policy-making and resource allocation.
It depends on the jurisdiction and purpose of data collection. In some regions, it may be required for healthcare or research purposes, while in others it may be optional but recommended for comprehensive analysis.
While there are privacy considerations, proper anonymization and compliance with data protection regulations (e.g., HIPAA, GDPR) can mitigate risks while ensuring the data remains useful for research and policy purposes.































