Health insurance ecodes, short for evaluation and management codes, are standardized numerical and alphanumeric codes used in the healthcare industry to document and bill for medical services provided to patients. These codes, primarily derived from the Current Procedural Terminology (CPT) and International Classification of Diseases (ICD) systems, play a crucial role in ensuring accurate reimbursement for healthcare providers, as they categorize the complexity and nature of patient encounters. By assigning specific ecodes based on factors such as patient history, examination, and medical decision-making, healthcare professionals can effectively communicate the level of care delivered, streamline administrative processes, and maintain compliance with insurance regulations. Understanding health insurance ecodes is essential for both providers and patients, as it directly impacts the financial aspects of healthcare delivery and the overall patient experience.
Explore related products

$44.02 $233.95





What You'll Learn
- Understanding E-Codes: Definition, purpose, and role in health insurance claims processing
- Types of E-Codes: Differentiating external cause codes in medical billing
- E-Code Accuracy: Importance of precise coding for claim approval and reimbursement
- Common E-Code Mistakes: Frequent errors and their impact on insurance claims
- E-Code Updates: Staying current with ICD coding changes for health insurance
![]()
Understanding E-Codes: Definition, purpose, and role in health insurance claims processing
E-codes, or external cause codes, are a critical yet often overlooked component of health insurance claims. These alphanumeric identifiers, part of the International Classification of Diseases (ICD) system, serve a distinct purpose: to capture the external circumstances leading to injury, poisoning, or other health conditions. Unlike diagnostic codes that describe the medical issue, E-codes provide context—the "how" and "why" behind the diagnosis. For instance, an E-code might specify whether a fracture resulted from a fall at home (E880.0) or a motor vehicle accident (V42.3). This granularity is essential for insurers, public health agencies, and healthcare providers to understand risk factors, allocate resources, and prevent future incidents.
Consider the claims processing workflow to grasp the role of E-codes. When a claim is submitted, the primary diagnosis code identifies the condition, but the E-code adds a layer of detail that influences adjudication. For example, a claim for a burn injury (T20.0) paired with an E-code indicating a workplace accident (E919.0) may trigger a review for occupational safety compliance or workers’ compensation eligibility. Insurers use this information to determine coverage, assess liability, and identify trends that could impact premiums or policy design. Without E-codes, claims processing would lack critical context, potentially leading to errors in reimbursement or missed opportunities for intervention.
The purpose of E-codes extends beyond claims processing to public health surveillance. By aggregating E-code data, health agencies can identify high-risk environments or activities, such as a surge in drowning incidents (E910.0) during summer months. This data informs targeted prevention programs, like pool safety campaigns or lifeguard training initiatives. For healthcare providers, E-codes also serve as a tool for patient education and risk mitigation. A physician might use an E-code for a pedestrian injured in traffic (V09.9) to counsel the patient on safer walking practices or advocate for improved crosswalk infrastructure in the community.
However, the effective use of E-codes requires precision and adherence to coding guidelines. Misapplication can lead to claim denials or skewed health data. For instance, using a nonspecific E-code like "other accidental poisoning" (E850.9) instead of a detailed code for a medication overdose (E935.0) could delay claim approval or obscure critical trends in drug safety. Providers and coders must stay updated on ICD revisions, as E-codes evolve to reflect emerging risks, such as vaping-related injuries (E64.2) or cyberbullying-induced mental health crises (E95.8). Training and auditing are essential to ensure accuracy and maximize the utility of E-codes in both clinical and administrative settings.
In summary, E-codes are more than just supplementary data—they are a bridge between medical diagnosis and real-world context. For insurers, they streamline claims processing and inform risk management. For public health, they drive prevention strategies. For providers, they enhance patient care and community advocacy. Mastering E-codes requires understanding their purpose, integrating them into workflows, and leveraging their insights to improve outcomes. As healthcare systems grow more data-driven, the role of E-codes will only become more pivotal, making them an indispensable skill for anyone involved in health insurance or patient care.
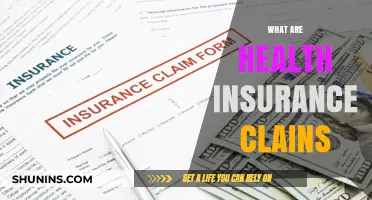
Medical Insurance: Where to Find the Right Information
You may want to see also
Explore related products






![]()
Types of E-Codes: Differentiating external cause codes in medical billing
E-Codes, or external cause codes, are essential in medical billing as they provide context for injuries, poisoning, and other health encounters tied to external factors. These codes, part of the ICD-10-CM system, fall under the "S" and "T" categories, but E-Codes specifically focus on the circumstances surrounding an event rather than the diagnosis itself. For instance, if a patient falls from a ladder, the E-Code would describe the location and mechanism of the fall, while the diagnosis code would detail the resulting injury, such as a fractured arm. Understanding the types of E-Codes is critical for accurate billing and ensuring proper reimbursement.
One key type of E-Code is the activity code, which identifies the action the patient was performing when the injury occurred. These codes are crucial for insurers to assess risk and determine coverage. For example, E-Code W01.01XA indicates a pedestrian injured in a collision with a pedestrian conveyance, while V97.33XA describes a cyclist injured in a traffic accident. Activity codes are particularly important in workers’ compensation claims, where the nature of the activity can influence liability. Billing specialists must pair these codes with the appropriate diagnosis to paint a complete picture of the incident.
Another critical category is place codes, which specify where the event occurred. These codes range from Y92.010 (bathroom) to Y92.250 (street, including crosswalk). Place codes are vital for insurers and public health agencies, as they help identify environmental risks and inform preventive measures. For instance, a high incidence of injuries coded Y92.140 (stairway) might prompt an investigation into building safety standards. When selecting a place code, billers should consider the most specific location available, as this enhances the accuracy of the claim.
Status codes are a lesser-known but equally important type of E-Code, focusing on the patient’s role or status during the event. For example, Y09.0 indicates that the patient was a passenger in a motor vehicle, while Y93.D0 specifies that the patient was a bystander. These codes are particularly useful in liability cases, as they clarify the patient’s involvement in the incident. Misapplying a status code can lead to claim denials or delays, so billers must cross-reference the patient’s medical record and incident report carefully.
Finally, external cause status codes provide additional context, such as whether the event was accidental, intentional, or due to undetermined intent. For instance, X74.9XXA denotes intentional self-harm by unspecified means, while Y09.9 indicates assault by unspecified means. These codes are critical for insurers to differentiate between covered and non-covered events, such as injuries sustained during illegal activities. Billers should exercise caution when assigning these codes, as they can have significant legal and financial implications for both the patient and the provider.
In summary, differentiating between types of E-Codes—activity, place, status, and external cause status—is essential for accurate medical billing. Each type serves a unique purpose, from describing the patient’s actions to clarifying the event’s circumstances. By mastering these distinctions, billing professionals can ensure compliance, maximize reimbursement, and contribute to better public health data. Always double-check the ICD-10-CM guidelines and consult with coding experts when in doubt, as precision in E-Code selection is non-negotiable.
Why Insurance Companies Exclude Natural Medicine: Uncovering the Coverage Gap
You may want to see also
Explore related products



![California Insurance Code [2025 Edition]](https://m.media-amazon.com/images/I/51XPT2DBfHL._AC_UY218_.jpg)


![]()
E-Code Accuracy: Importance of precise coding for claim approval and reimbursement
E-codes, or external cause codes, are essential in health insurance for accurately documenting the circumstances of injuries, poisoning, and other adverse effects. These codes provide context beyond the diagnosis, helping insurers understand the event’s nature, intent, and activity involved. For instance, an E-code might differentiate between a pedestrian injured in a traffic accident (V01.90) and a cyclist struck by a car (V12.90), directly impacting claim categorization and processing. Without precise E-coding, claims risk denial or delay, as insurers rely on this data to verify coverage eligibility and allocate costs appropriately.
Consider a scenario where a 45-year-old patient visits the ER after a fall during a recreational hike. The diagnosis code (S72.001A, nondisplaced fracture of right femur) is clear, but the E-code (W01.XXXA, fall on same level from slipping, tripping, or stumbling) specifies the mechanism and setting. If the coder mistakenly uses W03.XXXA (fall involving ice or snow), the insurer might question the claim’s validity, especially if the patient’s policy excludes adventure sports. This error could trigger a costly audit or reimbursement rejection, highlighting the need for coders to cross-reference patient charts, physician notes, and activity details meticulously.
The financial and operational stakes of E-code accuracy cannot be overstated. Insurers use these codes to identify trends, assess risk, and negotiate provider contracts. For example, a hospital with a high volume of W22.02 (struck by rugby ball) claims might be flagged for sports-related injury risks, influencing future premium calculations. Providers, meanwhile, face revenue cycle disruptions when claims are denied due to E-code discrepancies. A 2022 study found that 18% of denied orthopedic claims involved E-code errors, with an average correction time of 42 days—a delay that strains cash flow and administrative resources.
To improve E-code precision, coders should adopt a three-step verification process. First, review the physician’s documentation for keywords like “slipped,” “collided,” or “ingested,” which align with specific E-code categories. Second, cross-reference the patient’s age and activity (e.g., a 65-year-old with a hip fracture from a fall at home may warrant E-code W01.0XXA). Third, use coding software with built-in alerts for conflicting or incomplete codes. For instance, if a diagnosis indicates poisoning (T39.1X5A), the system should prompt for an E-code specifying accidental (X40-X49) vs. intentional (X60-X69) exposure.
Ultimately, E-code accuracy is a linchpin of the health insurance ecosystem, bridging clinical documentation and financial adjudication. Coders, providers, and insurers share responsibility for ensuring these codes reflect the true circumstances of each case. By prioritizing precision, stakeholders can minimize claim rejections, expedite reimbursements, and maintain trust in the healthcare billing process. As coding systems evolve, ongoing training and technological tools will be critical to keeping pace with complexity and compliance demands.
Contractor Medical Insurance: What You Need to Know
You may want to see also
Explore related products


![California Unemployment Insurance Code [2025 Edition]](https://m.media-amazon.com/images/I/513sESs2WkL._AC_UY218_.jpg)



![]()
Common E-Code Mistakes: Frequent errors and their impact on insurance claims
E-codes, or external cause codes, are essential in health insurance claims as they provide context for injuries, poisoning, and other health events. However, mistakes in their application can lead to claim denials, delays, or incorrect reimbursements. One frequent error is misclassifying the intent of injury, such as coding an accidental fall as intentional self-harm. For instance, using E-code E950-E959 (accidental poisoning by drugs) instead of E960-E969 (intentional self-poisoning) for a medication overdose can alter the claim’s outcome, especially if the insurer suspects misuse. This mistake often stems from incomplete patient histories or rushed coding, highlighting the need for thorough documentation and verification.
Another common pitfall is omitting the activity leading to the injury, which is crucial for E-codes like E880-E888 (accidents involving sports). For example, failing to specify whether a fracture occurred during a soccer match (E864.1) or a bicycle ride (E823.0) can result in claim rejections. Insurers rely on these details to assess risk and determine coverage, particularly in policies with exclusions for high-risk activities. Coders should cross-reference the patient’s account with medical records to ensure accuracy, as discrepancies can trigger audits or denials.
Inaccurate sequencing of E-codes is a third error with significant repercussions. E-codes must accompany the primary diagnosis code (e.g., a fracture) and follow a specific hierarchy. Placing an E-code before the injury code or failing to link it to the correct diagnosis can lead to underpayment or denial. For instance, coding S72.00XA (unspecified fracture of right femur) without the corresponding E-code W01.XXXA (fall on same level) leaves the claim incomplete. Training staff to understand the relationship between diagnosis and E-codes is critical to avoiding this mistake.
Lastly, ignoring age-specific guidelines can derail claims, particularly for pediatric or elderly patients. For example, using E915.0 (struck by motor vehicle) for a child without specifying playground equipment involvement (E915.4) overlooks key details insurers use to assess liability. Similarly, coding a fall in a nursing home (E885.0) as a generic slip (W19.XXXA) misses the institutional context, which may affect coverage. Tailoring E-codes to the patient’s demographic and environment ensures claims align with insurer expectations, reducing the risk of disputes.
To mitigate these errors, coders should adopt a three-step approach: verify the patient’s account, cross-reference medical records, and double-check code sequencing. Regular audits and staying updated on ICD-10 revisions can further minimize mistakes. By prioritizing accuracy in E-code application, healthcare providers can streamline claims processing, improve reimbursement rates, and enhance patient satisfaction.
Do Actors Have Health Insurance? Exploring Coverage in the Entertainment Industry
You may want to see also
Explore related products



$46.74 $49.99


![]()
E-Code Updates: Staying current with ICD coding changes for health insurance
Health insurance E-codes, officially known as external cause codes in the International Classification of Diseases (ICD) system, are essential for accurately documenting the circumstances of injuries, poisoning, and other adverse effects. These codes provide critical context for healthcare providers, insurers, and researchers, influencing claim approvals, epidemiological studies, and public health initiatives. However, the ICD system undergoes regular updates, making it imperative for professionals to stay current with E-code changes to ensure compliance and precision in coding.
Understanding the Impact of ICD Updates on E-Codes
Each ICD revision, such as the transition from ICD-9 to ICD-10 or future updates to ICD-11, introduces new E-codes, modifies existing ones, or retires outdated categories. For instance, ICD-10 expanded E-codes to include more specific scenarios, like Y92.XXX for the place of occurrence of an injury. Failing to adopt these changes can lead to claim denials, delayed reimbursements, or misclassified data. For example, using an ICD-9 E-code (E800-E999) in a system requiring ICD-10 (V00-Y99) would render the code invalid. Staying updated ensures that health insurance claims align with payer requirements and regulatory standards.
Practical Steps to Stay Current with E-Code Changes
To navigate ICD updates effectively, professionals should adopt a proactive approach. First, subscribe to official ICD coding resources, such as the Centers for Medicare & Medicaid Services (CMS) or the World Health Organization (WHO), which publish detailed guidelines and transition timelines. Second, participate in continuing education programs or webinars focused on ICD updates, particularly those highlighting E-code changes. Third, leverage coding software or tools that automatically integrate updated code sets, reducing the risk of human error. For instance, using a system that flags deprecated codes can prevent accidental misuse.
Cautions and Common Pitfalls in E-Code Updates
Despite best efforts, professionals may encounter challenges when implementing ICD updates. One common pitfall is assuming that E-codes function independently of other ICD codes. In reality, E-codes must accompany a primary diagnosis code (e.g., S72.001A for a femur fracture) to provide a complete clinical picture. Another issue is overlooking the specificity required by newer E-codes. For example, ICD-10 mandates coding the activity (Y93.XXX) and place (Y92.XXX) related to an injury, whereas ICD-9 did not. Ignoring these details can result in incomplete or inaccurate documentation.
Staying current with ICD coding changes for health insurance E-codes is not merely a compliance requirement but a cornerstone of effective healthcare administration. Accurate E-code usage ensures that claims are processed efficiently, data is reliable for research, and patient care is appropriately documented. By understanding the impact of updates, adopting practical strategies, and avoiding common pitfalls, professionals can maintain coding integrity and support the broader goals of healthcare systems. As ICD systems continue to evolve, ongoing vigilance and education will remain essential for mastering E-code updates.
Step-by-Step Guide to Applying for Military Health Insurance Coverage
You may want to see also
Frequently asked questions
Health insurance ecodes, or "evaluation codes," are standardized codes used to document and communicate the reason for a patient's visit, diagnosis, or procedure during a healthcare encounter. They help insurance companies understand the medical necessity of services provided.
Ecodes play a crucial role in health insurance claims as they justify the medical services rendered. Accurate ecodes ensure proper reimbursement from insurance providers, while incorrect or missing ecodes can lead to claim denials or delays.
No, ecodes are distinct from CPT (Current Procedural Terminology) and ICD (International Classification of Diseases) codes. While CPT codes describe procedures and ICD codes classify diagnoses, ecodes specifically focus on the reason for the patient's visit or the evaluation performed during the encounter.