The implementation of Medicare for All, a single-payer healthcare system, would significantly impact private health insurance in the United States. Under this proposal, a government-run program would provide comprehensive healthcare coverage to all citizens, potentially rendering private insurance plans redundant for many individuals. Currently, private health insurance companies operate alongside Medicare, offering various plans with different levels of coverage and costs. However, with Medicare for All, the role of private insurers might shift towards providing supplemental coverage for services not included in the universal plan, such as cosmetic procedures or private hospital rooms. This transition could lead to a substantial transformation in the healthcare industry, affecting insurance companies, healthcare providers, and consumers alike, as they navigate a new system where private insurance plays a different, potentially diminished, role.
| Characteristics | Values |
|---|---|
| Role of Private Insurance | Private insurance would become supplemental, covering services not included in Medicare for All, such as cosmetic procedures, private rooms, or additional benefits. |
| Cost to Consumers | Premiums for private supplemental insurance would likely decrease due to reduced administrative costs and narrower coverage scope. |
| Employer-Sponsored Insurance | Employer-sponsored health insurance would likely be phased out or significantly reduced, as Medicare for All would cover all essential healthcare needs. |
| Market Competition | Private insurers would shift focus to competing on supplemental plans, potentially increasing innovation in add-on services. |
| Administrative Costs | Overall administrative costs for private insurers could decrease due to simplified billing and reduced need for extensive provider networks. |
| Coverage Gaps | Private insurance could fill gaps in Medicare for All, such as dental, vision, or long-term care, which may not be fully covered under the public plan. |
| Consumer Choice | Consumers would have less choice in primary health insurance but more options for supplemental coverage tailored to individual needs. |
| Industry Impact | The private insurance industry would shrink in size but remain relevant for supplemental and niche markets. |
| Government Regulation | Private supplemental plans would still be subject to regulations to ensure fairness and prevent discriminatory practices. |
| Transition Period | A phased implementation of Medicare for All would allow private insurers time to adapt their business models to the new landscape. |
Explore related products






What You'll Learn
- Premium Changes: How Medicare for All affects private insurance premiums and out-of-pocket costs
- Coverage Gaps: Potential differences in coverage between private plans and Medicare for All
- Employer-Sponsored Plans: Impact on employer-provided health insurance under a single-payer system
- Supplemental Insurance: Role of private insurance as a supplement to Medicare for All
- Industry Transition: How private insurers adapt or phase out under Medicare for All
![]()
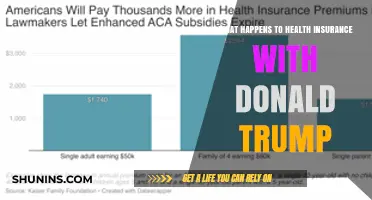
Premium Changes: How Medicare for All affects private insurance premiums and out-of-pocket costs
Under a Medicare for All system, private insurance premiums would likely decrease significantly, but the shift in cost structure demands careful consideration. Currently, private insurers spread costs across a risk pool, often resulting in high premiums for comprehensive coverage. With Medicare for All, the federal government assumes the primary funding role, eliminating the need for profit margins and administrative overhead associated with private plans. This could reduce premiums by 20-40% for individuals who choose to retain supplemental private insurance, according to estimates from the Urban Institute. However, these savings depend on the design of the public plan and whether it covers all services currently offered by private insurers.
Out-of-pocket costs present a more complex scenario. Medicare for All proposals typically eliminate deductibles and copays for essential services, potentially saving households thousands annually. For instance, a family of four with an employer-sponsored plan currently spends an average of $5,700 yearly on out-of-pocket costs, per Kaiser Family Foundation data. Under a robust public option, this could drop to near zero for primary care and preventive services. Yet, supplemental private plans might reintroduce cost-sharing for non-essential services like cosmetic procedures or premium hospital rooms, creating a tiered system where out-of-pocket expenses persist for those seeking additional coverage.
Employer-sponsored insurance (ESI), which covers 155 million Americans, would undergo a dramatic transformation. Premiums for supplemental private plans tied to ESI could become more affordable due to reduced risk pooling needs, but employers might shift contributions to wages instead. For example, a worker paying $1,200 annually toward a family plan might see this cost halved, with the employer redirecting savings into salary increases. However, this trade-off requires clear communication to avoid perceptions of benefit loss, as employees may not immediately equate wage adjustments with healthcare savings.
For individuals purchasing private insurance on the individual market, premium reductions could be even more pronounced. Current average monthly premiums of $456 (HealthCare.gov) might drop to $200-$300 for supplemental plans, depending on coverage scope. Yet, out-of-pocket costs for specialized care could rise if private plans focus on niche services excluded from the public option. For instance, a policy covering advanced cancer treatments might carry a $500 deductible and 20% coinsurance, requiring careful plan selection to align with health needs.
In conclusion, Medicare for All would reshape premium and out-of-pocket dynamics, offering lower overall costs for most but introducing variability based on supplemental coverage choices. Policymakers must balance public plan comprehensiveness with private market incentives to ensure affordability without compromising access. Individuals should prepare to evaluate supplemental plans critically, focusing on coverage gaps and cost-sharing structures to optimize financial protection in a post-Medicare for All landscape.
No Health Insurance in NJ? Consequences and Options Explained
You may want to see also
Explore related products






![]()
Coverage Gaps: Potential differences in coverage between private plans and Medicare for All
Private health insurance plans often cover services that Medicare for All might exclude, creating potential gaps in care. For instance, many private plans offer comprehensive dental, vision, and hearing coverage, while Medicare for All proposals typically limit these benefits to specific age groups or conditions. A 65-year-old with a private plan might receive annual dental cleanings and hearing aids, but under Medicare for All, they could face out-of-pocket costs for these services unless deemed medically necessary. This disparity highlights the need for individuals to assess their current coverage and anticipate future needs.
Consider the case of prescription drug coverage. Private plans frequently include access to newer, brand-name medications with lower copays, whereas Medicare for All might prioritize generic alternatives to control costs. For a patient requiring a specialty drug for a chronic condition, this shift could mean higher out-of-pocket expenses or limited treatment options. To mitigate this, individuals should review their medication regimens and explore supplemental coverage options if Medicare for All becomes a reality.
Another critical area is long-term care. Private insurance often provides coverage for in-home care, assisted living, or nursing home stays, but Medicare for All typically excludes these services unless they meet strict medical criteria. A family planning for an aging relative’s care might find themselves underinsured, requiring additional savings or alternative arrangements. Proactive financial planning and understanding the limitations of Medicare for All are essential to avoid unexpected costs.
Finally, private plans frequently offer access to a broader network of providers, including specialists and out-of-state care, while Medicare for All could restrict provider choice to control expenses. A patient seeking a second opinion from a renowned specialist might face barriers under a single-payer system. To navigate this, individuals should research provider networks and consider the trade-offs between cost and access when evaluating their healthcare options.
In summary, while Medicare for All aims to provide universal coverage, it may introduce gaps in areas like dental, vision, prescription drugs, long-term care, and provider access compared to private plans. By understanding these potential differences, individuals can make informed decisions to ensure continuity of care and financial stability.
Medical Pedicures: Are They Covered by Insurance?
You may want to see also
Explore related products






![]()
Employer-Sponsored Plans: Impact on employer-provided health insurance under a single-payer system
Under a Medicare for All system, employer-sponsored health insurance would undergo a seismic shift, fundamentally altering the role of businesses in healthcare provision. Currently, over half of Americans receive health coverage through their employers, a system that has become deeply entrenched in the U.S. labor market. However, a single-payer model would render this arrangement obsolete, as comprehensive healthcare would be guaranteed to all citizens regardless of employment status. This raises critical questions about the financial and operational implications for employers, as well as the broader economic consequences of dismantling a system that has long been a cornerstone of employee benefits.
From a financial perspective, employers would experience significant cost savings by shedding the burden of health insurance premiums. In 2020, the average annual premium for employer-sponsored family coverage exceeded $21,000, with employers contributing roughly 70% of this amount. Under Medicare for All, these funds could be redirected toward wage increases, expanded benefits, or reinvestment in business operations. For instance, a mid-sized company with 500 employees could potentially reallocate upwards of $7 million annually, assuming current contribution levels. However, this transition would require careful planning to avoid employee backlash, as workers may perceive the loss of employer-sponsored insurance as a reduction in overall compensation.
Operationally, the elimination of employer-sponsored plans would streamline HR processes, as businesses would no longer need to manage complex benefits packages, negotiate with insurers, or administer open enrollment periods. This could free up resources and reduce administrative overhead, particularly for small and medium-sized enterprises (SMEs) that often lack dedicated benefits specialists. However, employers would need to navigate new compliance requirements, such as ensuring payroll systems accurately reflect tax adjustments related to healthcare funding. For example, a Medicare for All system might involve higher payroll taxes, necessitating updates to payroll software and employee communication strategies.
A comparative analysis of international models provides insight into potential outcomes. In Canada, where a single-payer system exists, employers have shifted focus to supplemental benefits like dental, vision, and wellness programs. Similarly, U.S. employers might pivot toward offering enhanced voluntary benefits to remain competitive in the labor market. For instance, companies could provide access to concierge medicine, mental health services, or fitness subsidies to attract and retain talent. This approach would allow businesses to maintain their role in employee well-being while adapting to the new healthcare landscape.
In conclusion, the transition to a single-payer system would redefine the relationship between employers and healthcare, offering both opportunities and challenges. While financial savings and operational efficiencies are compelling, employers must proactively address employee concerns and adapt their benefits strategies. By learning from international examples and planning strategically, businesses can navigate this shift effectively, ensuring a smooth transition for their workforce while capitalizing on the newfound flexibility in resource allocation.
GOP Policies: Millions Lose Health Insurance Coverage - What's Next?
You may want to see also
Explore related products






![]()
Supplemental Insurance: Role of private insurance as a supplement to Medicare for All
Under a Medicare for All system, private health insurance would no longer serve as the primary coverage for most Americans. However, this doesn't mean private insurance disappears entirely. Instead, its role shifts to providing supplemental coverage, filling gaps left by the standardized benefits of a single-payer system.
Imagine Medicare for All as a sturdy foundation, guaranteeing essential healthcare services for everyone. Supplemental private insurance then becomes the customizable layer, allowing individuals to tailor their coverage to their specific needs and preferences.
This shift has significant implications. Premiums for supplemental plans would likely be lower than current private insurance costs, as they wouldn't need to cover the entire spectrum of healthcare expenses. This could make specialized coverage more accessible, particularly for those with chronic conditions or those seeking enhanced benefits like dental, vision, or alternative therapies.
Let's consider a practical example. A 65-year-old retiree with Medicare for All might opt for a supplemental plan that covers prescription drug costs beyond the standard formulary, ensuring access to specific medications not fully covered by the base plan. Similarly, a young professional might choose a supplemental plan offering comprehensive mental health coverage, including access to specialized therapists and alternative treatment modalities.
The key advantage of this model lies in its flexibility. Individuals can choose the level of supplemental coverage that aligns with their health status, lifestyle, and budget. This personalized approach empowers individuals to take control of their healthcare, ensuring they have the protection they need without paying for unnecessary services.
However, it's crucial to address potential challenges. Clear regulations would be necessary to prevent supplemental plans from discriminating against individuals with pre-existing conditions or engaging in practices that undermine the equity principles of Medicare for All. Additionally, ensuring transparency in pricing and benefits is essential to allow consumers to make informed choices.
In conclusion, the role of private insurance under Medicare for All would transform from a primary coverage provider to a specialized supplement. This shift offers the potential for greater accessibility, customization, and control over healthcare choices. By carefully addressing regulatory concerns, we can ensure that supplemental insurance enhances the benefits of a universal healthcare system, providing a safety net for all while allowing individuals to tailor their coverage to their unique needs.
Why Insurance Companies Ask About Your Home Heating System
You may want to see also
Explore related products






![]()
Industry Transition: How private insurers adapt or phase out under Medicare for All
Private insurers face an existential crossroads under Medicare for All, a policy that would fundamentally reshape the U.S. healthcare landscape. The traditional role of private insurance—managing risk, negotiating provider rates, and administering benefits—would be largely usurped by a single-payer system. Yet, rather than an abrupt extinction, the industry’s transition is more likely to involve strategic adaptation, with insurers pivoting to fill gaps left by a government-run program. For instance, supplemental plans covering services like dental, vision, or concierge care could become their new niche, mirroring the role of Medigap policies today. This shift would require insurers to rethink their value proposition, moving from primary coverage providers to specialized service enhancers.
To navigate this transition, insurers must first assess their operational strengths and market positioning. Companies with robust administrative infrastructures, like UnitedHealth Group, could leverage their expertise to manage Medicare for All claims processing or fraud detection on behalf of the government. Others might focus on employer-sponsored wellness programs, which could remain outside the scope of a single-payer system. A cautionary note: insurers that fail to innovate risk becoming irrelevant, as seen in countries like Canada, where private insurers primarily offer supplemental coverage rather than competing with the public system.
A persuasive argument for insurers’ survival lies in their ability to address Medicare for All’s limitations. For example, long wait times for elective procedures under single-payer systems in other countries have driven demand for private alternatives. Insurers could capitalize on this by offering expedited access to specialists or premium hospital networks, albeit at a cost. This tiered model, already seen in the UK’s NHS, allows private insurers to coexist with public healthcare by catering to consumers willing to pay for added convenience or quality.
Comparatively, the pharmaceutical industry’s response to Medicare Part D provides a useful analogy. When the program launched in 2006, drug manufacturers adapted by offering discount programs and partnering with insurers to manage formularies. Similarly, private insurers under Medicare for All could partner with providers to create value-based care models, ensuring efficient delivery of services not fully covered by the government. Such collaborations would require insurers to shift from fee-for-service to outcomes-based reimbursement, a transition already underway in parts of the industry.
In conclusion, the phase-out of private insurers as primary healthcare providers under Medicare for All is not inevitable. Instead, the industry’s survival hinges on its ability to innovate, specialize, and collaborate. By focusing on supplemental coverage, administrative services, and value-added offerings, insurers can carve out a sustainable role in a single-payer ecosystem. The key takeaway for industry leaders: adaptability, not resistance, will determine their relevance in a post-Medicare for All world.
HSA Contributions: Medical Insurance Expense or Not?
You may want to see also
Frequently asked questions
Medicare for All aims to provide universal healthcare coverage, potentially reducing the need for private insurance. However, some private plans might still exist for supplemental coverage not included in the government plan.
It depends on the specific legislation. Some proposals may allow private insurance to coexist, while others might restrict or phase it out entirely in favor of the government-run system.
Medicare for All would likely eliminate private insurance premiums, as the system would be funded through taxes. However, the overall financial impact would depend on tax adjustments and individual circumstances.
Under Medicare for All, employers would no longer need to provide health insurance as a benefit, as coverage would be universal. Employer contributions might shift to supporting the government-funded system instead.








![Life and Health Insurance Study Cards: Life Health Insurance License Exam Prep with Practice Test Questions [Full Color]](https://m.media-amazon.com/images/I/51Pox87Z5lL._AC_UL320_.jpg)