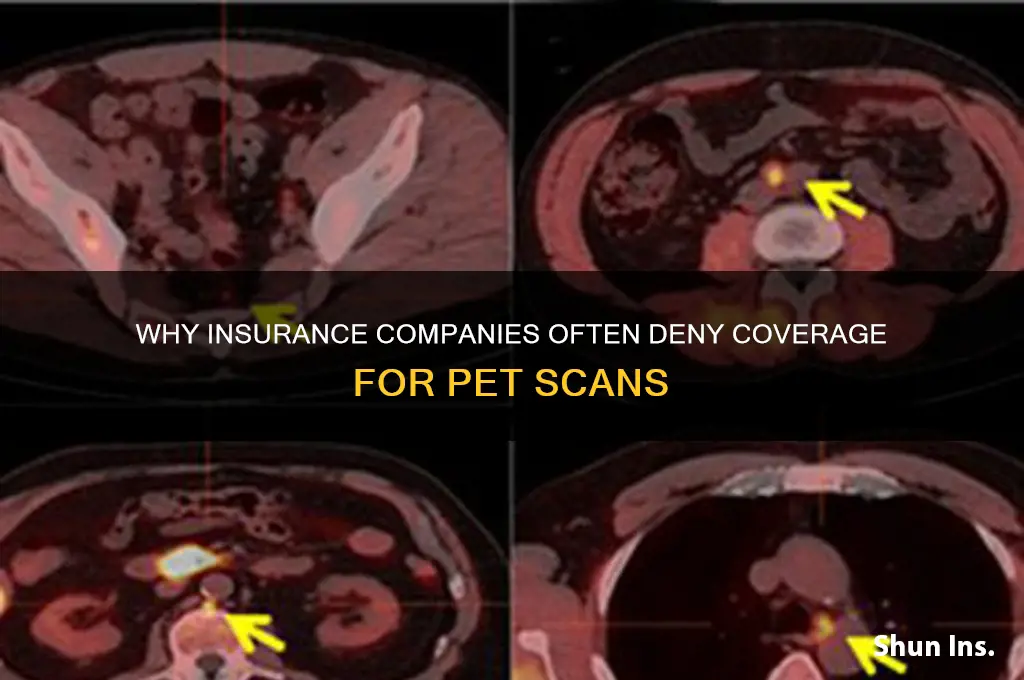
Insurance companies often deny coverage for PET scans due to their high cost and the perception that they may not always be medically necessary. While PET scans are highly effective in diagnosing and monitoring conditions like cancer, insurers frequently require strict criteria to be met before approving the procedure. These criteria often include evidence that the scan will significantly impact treatment decisions or that other, less expensive imaging methods have already been exhausted. Additionally, some insurance plans may classify PET scans as experimental or investigational for certain conditions, further limiting their approval. The denial of coverage can also stem from concerns about overutilization, as insurers aim to balance patient care with cost management, leading to disputes between healthcare providers and insurance companies over the appropriateness of the procedure.
| Characteristics | Values |
|---|---|
| High Cost | PET scans are expensive, often costing $1,000 to $5,000 per scan. |
| Limited Medical Necessity | Insurers may deny coverage if they deem the scan not medically necessary. |
| Alternative Options Available | Cheaper imaging tests like CT or MRI may be preferred by insurers. |
| Lack of Clear Guidelines | Ambiguity in medical guidelines can lead to denials. |
| Pre-Authorization Requirements | Failure to obtain pre-authorization can result in denial. |
| Experimental or Investigational Use | Insurers may deny coverage if the scan is considered experimental. |
| Policy Exclusions | Some policies explicitly exclude PET scans from coverage. |
| Frequency of Requests | Repeated requests for PET scans may be denied as unnecessary. |
| Provider Network Restrictions | Out-of-network providers may not be covered for PET scans. |
| Patient-Specific Factors | Denials can occur based on the patient's condition or history. |
| Insurance Plan Type | HMOs or basic plans may offer less coverage for advanced imaging. |
| Lack of Supporting Documentation | Insufficient medical records or evidence can lead to denial. |
| Regional Variations | Coverage policies may differ by state or region. |
| Cost-Benefit Analysis | Insurers may deny if the cost outweighs the perceived benefit. |
| Technology Advancements | Rapid advancements may lead to delays in coverage updates. |
Explore related products






What You'll Learn
- Lack of medical necessity criteria for PET scan requests
- Insufficient evidence supporting PET scan diagnostic value in specific cases
- High cost of PET scans versus perceived clinical benefit
- Policy exclusions for experimental or investigational procedures
- Incomplete or inaccurate documentation in the patient’s medical records
![]()
Lack of medical necessity criteria for PET scan requests
Insurance companies often deny PET scan requests due to a perceived lack of medical necessity, a criterion that hinges on whether the procedure is essential for diagnosis, treatment planning, or monitoring. This determination is not arbitrary; it is rooted in evidence-based guidelines established by medical societies and regulatory bodies. For instance, the American College of Radiology (ACR) and the Society of Nuclear Medicine and Molecular Imaging (SNMMI) provide appropriateness criteria for PET scans in various clinical scenarios, such as oncology, neurology, and cardiology. When a request does not align with these guidelines, insurers may deny coverage, citing insufficient justification for the scan’s utility in the patient’s specific case.
Consider a 65-year-old patient with stage II lung cancer who has already undergone surgery and is being monitored for recurrence. A PET scan request in this scenario might be denied if the patient is asymptomatic and has no clinical or radiological evidence of disease progression. According to ACR guidelines, routine surveillance PET scans in this context are not recommended unless there is a specific clinical indication, such as rising tumor markers or suspicious findings on other imaging studies. Without meeting these criteria, the scan is deemed unnecessary, leading to denial.
To navigate this challenge, healthcare providers must ensure that PET scan requests are accompanied by detailed clinical documentation that clearly outlines the medical necessity. This includes specifying the patient’s diagnosis, current symptoms, prior imaging results, and how the PET scan will directly impact treatment decisions. For example, in a patient with lymphoma, a PET scan might be justified to assess treatment response after chemotherapy, as it provides critical information for adjusting therapy. However, if the request lacks this level of specificity, insurers are likely to deny it, viewing the scan as investigational rather than essential.
A comparative analysis reveals that denials often stem from a mismatch between the requested procedure and the patient’s clinical profile. For instance, while PET scans are highly effective in staging advanced cancers, they may offer limited value in early-stage diseases where other, less costly imaging modalities suffice. Insurers prioritize cost-effectiveness, and when a PET scan does not demonstrably improve patient outcomes over alternative options, it falls outside the scope of medical necessity. This underscores the importance of aligning requests with both clinical guidelines and the patient’s individual needs.
Practically, providers can reduce denials by adopting a proactive approach. This includes staying updated on evolving appropriateness criteria, engaging in peer-to-peer reviews with insurers to discuss complex cases, and utilizing decision-support tools integrated into electronic health records. For patients, understanding the criteria for PET scan approval can help manage expectations and facilitate informed discussions with their healthcare team. By bridging the gap between clinical practice and insurer requirements, both providers and patients can increase the likelihood of PET scan approval when it is truly warranted.
Understanding Blue Book Values: Which One Do Insurers Use for Totaled Cars?
You may want to see also
Explore related products






![]()
Insufficient evidence supporting PET scan diagnostic value in specific cases
Insurance companies often deny coverage for PET scans due to a lack of robust evidence supporting their diagnostic value in certain medical scenarios. This decision is rooted in the principle of cost-effectiveness, where treatments and tests must demonstrate clear benefits to justify their expense. For instance, in early-stage breast cancer, PET scans are frequently deemed unnecessary because mammograms and ultrasounds provide sufficient information for diagnosis and treatment planning. The added cost of a PET scan, which can range from $1,000 to $3,000, is not supported by evidence of improved outcomes in this context. This highlights a critical gap between technological capability and clinical necessity.
Consider the case of prostate cancer, where PET scans using PSMA tracers have shown promise in detecting metastases. However, for patients with low-risk, localized disease, the diagnostic yield of PET scans is minimal. Studies indicate that only 5-10% of these patients benefit from the additional information provided by a PET scan, which is insufficient to warrant routine use. Insurance companies rely on such data to make coverage decisions, prioritizing interventions with higher impact. For patients and providers, understanding this evidence-based approach is crucial when advocating for PET scans in specific cases.
A persuasive argument for PET scan denial often centers on the absence of long-term outcome data. For example, in non-small cell lung cancer, while PET scans can identify distant metastases, their impact on survival rates remains unclear. Clinical trials have yet to conclusively demonstrate that early detection of metastases via PET scans leads to better treatment outcomes or prolonged survival. Without this evidence, insurers view PET scans as investigational rather than standard of care, leading to denials. This underscores the need for ongoing research to bridge the evidence gap.
Comparatively, PET scans are more widely accepted in advanced cancers, such as lymphoma, where they play a pivotal role in staging and monitoring treatment response. However, in early-stage or indolent conditions, their utility is less defined. For instance, in multiple myeloma, PET scans are not routinely recommended for initial diagnosis due to limited evidence of their superiority over conventional imaging methods like MRI or CT. This disparity in evidence across disease stages and types complicates coverage decisions, leaving patients and providers to navigate a complex landscape of approvals and denials.
To address denials effectively, patients and providers should focus on building a case based on individualized clinical need. This includes documenting symptoms, progression, or complications that standard imaging fails to capture. For example, if a patient with recurrent colorectal cancer has rising tumor markers but negative CT results, a PET scan could be justified to locate occult metastases. Providing such specific, case-based evidence increases the likelihood of insurance approval, even in scenarios where general guidelines do not support PET scan use. This tailored approach bridges the gap between broad evidence and unique patient circumstances.
Unemployed and Uninsured: Getting Covered Without Income
You may want to see also
Explore related products






![]()
High cost of PET scans versus perceived clinical benefit
PET scans, while invaluable in certain medical scenarios, carry a hefty price tag—often ranging from $3,000 to $6,000 per scan in the United States. This cost is a significant factor in insurance companies’ reluctance to approve them. For instance, a Medicare analysis revealed that PET scans for Alzheimer’s disease, which cost approximately $3,000 each, were denied in over 60% of cases due to insufficient evidence of clinical benefit. The financial burden on insurers, coupled with the limited diagnostic yield in some cases, creates a natural tension between accessibility and fiscal responsibility.
Consider the clinical benefit of PET scans in lung cancer staging. While they can detect metastases with high accuracy, studies show that in early-stage non-small cell lung cancer (NSCLC), PET scans alter treatment plans in only 10-15% of cases. This raises the question: is the high cost justified when the scan’s impact on patient management is relatively modest? Insurers often weigh this marginal benefit against the expense, opting for more cost-effective alternatives like CT scans, which, while less sensitive, are significantly cheaper at $300-$700 per scan.
From a persuasive standpoint, the argument for PET scan approval hinges on its potential to improve patient outcomes in specific, high-impact scenarios. For example, in recurrent colorectal cancer, PET scans can identify distant metastases missed by CT, leading to more targeted therapies. However, insurers argue that such cases are the exception rather than the rule. Without clear guidelines on when PET scans provide definitive clinical value, insurers default to denial, prioritizing cost containment over potential—but uncertain—benefits.
A comparative analysis highlights the disparity in cost-effectiveness across different medical technologies. For instance, mammograms, which cost around $150-$250, have a well-established role in breast cancer screening, with proven benefits in early detection and survival. In contrast, PET scans lack such universal applicability, often being limited to specific cancer types or stages. This disparity underscores why insurers are more likely to approve mammograms while denying PET scans, even when patients and providers advocate for their use.
Practically speaking, patients and providers can improve the likelihood of PET scan approval by documenting clear clinical justification. For example, in cases of suspected lymphoma recurrence, detailing symptoms, lab abnormalities, and prior treatment responses can strengthen the case for a PET scan. Additionally, understanding insurer-specific criteria—such as requiring a prior CT scan or biopsy—can streamline the pre-authorization process. While the high cost remains a barrier, proactive measures can bridge the gap between perceived clinical benefit and insurer approval.
Why Company Health Insurance Costs Skyrocket: Uncovering the Expensive Truth
You may want to see also
Explore related products






![]()
Policy exclusions for experimental or investigational procedures
Insurance companies often deny coverage for PET scans by classifying them as experimental or investigational procedures, a designation rooted in policy exclusions designed to manage costs and ensure evidence-based care. These exclusions hinge on whether a procedure has been proven safe, effective, and widely accepted in the medical community. For PET scans, this classification can vary depending on the condition being diagnosed or monitored. For instance, while PET scans are considered standard for staging certain cancers like lymphoma or lung cancer, they may be deemed investigational for less common conditions like early-stage prostate cancer or neurological disorders. This distinction is not arbitrary; it’s based on clinical guidelines, peer-reviewed studies, and regulatory approvals, which insurers use to justify denials.
To navigate these exclusions, patients and providers must understand the criteria insurers use to define "experimental." Insurers often rely on third-party organizations like the Blue Cross Blue Shield Association (BCBSA) or the Centers for Medicare & Medicaid Services (CMS) to determine coverage policies. For example, CMS covers PET scans for specific indications, such as Alzheimer’s disease diagnosis or certain cancers, but excludes others, like chronic fatigue syndrome or fibromyalgia. Patients can improve their chances of approval by ensuring their condition aligns with these approved indications and by providing supporting documentation, such as clinical trial data or physician statements, to demonstrate medical necessity.
A persuasive argument for coverage lies in challenging the "experimental" label by highlighting the procedure’s established benefits. For instance, PET scans can detect cancer recurrence earlier than CT or MRI scans, potentially improving treatment outcomes. In a comparative analysis, a study published in the *Journal of Clinical Oncology* found that PET scans reduced unnecessary surgeries in patients with suspected recurrent colorectal cancer by 45%. Armed with such evidence, patients and providers can appeal denials by demonstrating that the procedure is not merely experimental but a critical tool for accurate diagnosis and treatment planning.
Practical tips for avoiding denials include verifying coverage before scheduling a PET scan and obtaining preauthorization from the insurer. Patients should ask their healthcare provider to submit a detailed request outlining the medical necessity, including symptoms, prior test results, and relevant clinical guidelines. For example, if a patient with non-small cell lung cancer needs a PET scan for staging, the request should cite the National Comprehensive Cancer Network (NCCN) guidelines, which recommend PET scans as a standard tool. Additionally, patients can consult their state’s insurance commissioner or seek assistance from patient advocacy groups to navigate appeals processes effectively.
In conclusion, policy exclusions for experimental or investigational procedures are a significant barrier to PET scan coverage, but they are not insurmountable. By understanding the criteria insurers use, gathering evidence of the procedure’s efficacy, and following practical steps to ensure compliance with coverage policies, patients and providers can increase the likelihood of approval. This proactive approach not only reduces the financial burden on patients but also ensures access to potentially life-saving diagnostic tools.
Join Ohio Insurance Panels: A Guide
You may want to see also
Explore related products






![]()
Incomplete or inaccurate documentation in the patient’s medical records
Incomplete or inaccurate documentation in a patient’s medical records is a silent saboteur of PET scan approvals. Insurance companies rely on these records to assess medical necessity, and gaps or errors can trigger denials. For instance, a missing diagnosis code, such as ICD-10 C50.9 (malignant neoplasm of breast, unspecified site), can leave insurers questioning the rationale for the scan. Without clear, consistent documentation linking symptoms to a specific condition, insurers may deem the procedure investigational rather than essential.
Consider a 62-year-old patient with a history of lung cancer presenting with unexplained weight loss and fatigue. If the oncologist’s notes fail to mention recent tumor marker elevations (e.g., CEA levels >5 ng/mL) or imaging findings suggestive of metastasis, the insurer may deny the PET scan as premature. Accurate documentation should include details like the stage of cancer (e.g., Stage IIIB), prior treatments (e.g., 6 cycles of carboplatin/pemetrexed), and the clinical suspicion of recurrence. Omitting these specifics creates ambiguity, leading insurers to question whether the scan is truly medically necessary.
Persuasive documentation is not just about completeness but also clarity. Vague terms like “possible recurrence” or “concern for metastasis” lack the specificity insurers demand. Instead, providers should use definitive language supported by objective data, such as “PET scan ordered to evaluate FDG-avid lesions seen on recent CT scan in a patient with biopsy-proven adenocarcinoma.” This approach bridges the gap between clinical suspicion and insurer criteria, reducing the likelihood of denial.
To avoid denials, providers must treat documentation as a strategic tool. Start by ensuring all diagnostic tests, such as biopsies or bloodwork, are linked explicitly to the patient’s condition. For example, note how a PSA level of 20 ng/mL in a prostate cancer patient justifies staging with a PET scan. Additionally, cross-reference prior imaging reports and consult notes to maintain consistency. Practical tips include using templates for common scenarios, double-checking ICD-10 and CPT codes (e.g., 78459 for PET scan of whole body), and involving medical coders to review records before submission.
The takeaway is clear: incomplete or inaccurate documentation is a preventable barrier to PET scan approvals. By treating medical records as a narrative that insurers must follow, providers can transform denials into approvals. Every detail matters—from the precise diagnosis to the rationale for the scan—because insurers scrutinize records for any reason to deny coverage. In this high-stakes game, thoroughness isn’t optional; it’s essential.
Secondary Medical Insurance: Can They Cancel You?
You may want to see also
Frequently asked questions
Insurance companies may deny PET scans if they deem the procedure medically unnecessary, experimental, or not aligned with established treatment guidelines for the diagnosed condition.
While PET scans are more costly than some imaging tests, insurance denials are often based on medical necessity rather than cost alone, though financial considerations may play a role in coverage decisions.
Yes, coverage for PET scans varies by cancer type and stage. Some insurers only approve them for advanced or recurrent cancers, while denying them for early-stage diagnoses or certain cancer types.
No, even with a doctor’s recommendation, insurance companies may deny coverage if they determine the scan does not meet their criteria for medical necessity or evidence-based guidelines.
Patients can appeal the denial by providing additional medical documentation, requesting a peer-to-peer review with the insurer’s physician, or seeking assistance from a patient advocate or attorney.































