Health insurance companies often create barriers to accessing healthcare through complex policies, high out-of-pocket costs, and stringent pre-authorization requirements, which can delay or deny necessary treatments. These practices, driven by profit motives, prioritize financial gain over patient well-being, leaving many individuals struggling to afford or navigate the system. Additionally, narrow provider networks and frequent policy changes further complicate access, disproportionately affecting vulnerable populations and exacerbating healthcare disparities. As a result, patients often face unnecessary hurdles, leading to delayed care, worsened health outcomes, and increased frustration with the healthcare system.
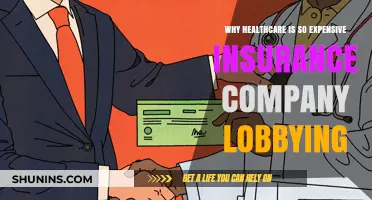
| Characteristics | Values |
|---|---|
| Prior Authorization Requirements | 90% of physicians report spending significant time on prior authorizations, delaying patient care (AMA, 2023) |
| Narrow Networks | 40% of ACA marketplace plans have narrow networks, limiting provider choice (Kaiser Family Foundation, 2023) |
| High Deductibles and Cost-Sharing | Average deductible for individual plans: $4,869 (KFF, 2023). 29% of insured adults report delaying care due to cost (Commonwealth Fund, 2022) |
| Denial of Claims | 1 in 5 medical claims are initially denied (AMA, 2022) |
| Step Therapy Protocols | 62% of physicians report step therapy requirements delaying access to necessary medications (AMA, 2023) |
| Utilization Management | Insurers use algorithms and reviews to limit care, often overriding physician recommendations (The New York Times, 2023) |
| Lack of Transparency | Complex pricing structures and hidden fees make it difficult for patients to understand costs (JAMA, 2022) |
| Administrative Burden | Physicians spend 15-30% of their time on insurance-related paperwork (AMA, 2023) |
| Profit-Driven Model | Top 5 health insurers made $45 billion in profit in 2022 (Statista, 2023) |
Explore related products






What You'll Learn
- Prior Authorization Delays: Requiring pre-approval for treatments slows access and complicates care
- Narrow Networks: Limited provider lists restrict patient choice and increase out-of-pocket costs
- High Deductibles: Steep out-of-pocket costs deter patients from seeking necessary medical care
- Claim Denials: Frequent rejections of valid claims force patients to fight for coverage
- Complex Policies: Confusing terms and conditions make it hard for patients to understand benefits
![]()
Prior Authorization Delays: Requiring pre-approval for treatments slows access and complicates care
Prior authorization, a process where health insurance companies require pre-approval for certain treatments, has become a significant barrier to timely and effective healthcare. Imagine a 45-year-old patient with rheumatoid arthritis prescribed a biologic medication like adalimumab (Humira). Before starting this $5,000-per-month treatment, their doctor must submit a prior authorization request, detailing the patient’s medical history, previous treatments, and the rationale for this specific drug. This bureaucratic step, which can take days or even weeks, delays relief for a patient already suffering from joint pain and inflammation. The irony? The insurer’s goal is ostensibly to ensure cost-effectiveness, yet the delay often worsens the patient’s condition, potentially leading to higher long-term costs.
Consider the process itself: a physician’s office spends an average of 14.1 hours per week on prior authorization tasks, according to the American Medical Association. This time could be spent on patient care instead. For instance, a primary care physician might need to prescribe a specific dosage of a cholesterol-lowering statin, such as 40 mg of atorvastatin, for a 60-year-old patient with a history of heart disease. The prior authorization form requires not only the diagnosis but also proof of failure on a cheaper alternative, like 20 mg of simvastatin. If the insurer denies the request, the doctor must appeal, further delaying treatment. This back-and-forth not only frustrates providers but also leaves patients in limbo, often forcing them to pay out-of-pocket or go without necessary care.
The impact of these delays extends beyond individual cases. A 2019 study in *JAMA Network Open* found that 90% of physicians reported that prior authorization led to treatment abandonment by patients. For example, a 30-year-old with depression might be prescribed a newer antidepressant like vortioxetine (Trintellix), but the insurer insists on a trial of fluoxetine (Prozac) first. If the patient doesn’t respond to fluoxetine, they must wait weeks for the prior authorization for vortioxetine to be approved. During this delay, their mental health could deteriorate, increasing the risk of hospitalization or worse. The system, designed to control costs, inadvertently prioritizes financial considerations over patient well-being.
To navigate this maze, patients and providers can take proactive steps. First, physicians should document all treatment decisions thoroughly, ensuring the prior authorization request includes detailed clinical justification. Patients can advocate for themselves by contacting their insurer’s patient advocate or using tools like the Prior Authorization Wizard, a free resource that streamlines the process. Additionally, state legislatures are increasingly passing laws to limit prior authorization delays; patients can support these efforts by contacting their representatives. While prior authorization isn’t going away, awareness and action can mitigate its most harmful effects, ensuring that care isn’t held hostage to red tape.
Ways to Verify Active Medical Insurance Coverage
You may want to see also
Explore related products


$167.66 $245.95




![]()
Narrow Networks: Limited provider lists restrict patient choice and increase out-of-pocket costs
Health insurance plans with narrow networks limit patients to a select group of healthcare providers, often excluding top-rated specialists and hospitals. This restriction is a strategic cost-cutting measure for insurers, but it comes at a steep price for consumers. Imagine needing a cardiologist for a complex heart condition, only to discover that none of the region’s leading experts are in-network. You’re forced to choose between suboptimal care or paying exorbitant out-of-pocket fees to see the specialist you need. This scenario isn’t hypothetical—it’s a growing reality for millions of Americans.
Consider the mechanics of narrow networks. Insurers negotiate lower rates with a smaller pool of providers, reducing their own expenses. In exchange, these providers agree to accept lower reimbursements, often limiting their ability to invest in advanced treatments or hire additional staff. Patients, meanwhile, face a double bind: their choices are artificially constrained, and if they opt for out-of-network care, they may incur costs that rival the price of a small car. For instance, a routine MRI that might cost $500 in-network could soar to $2,000 or more out-of-network, even with insurance coverage.
The impact of narrow networks extends beyond financial strain. Limited provider lists can delay critical care, particularly for patients with chronic or rare conditions. A study by the *Journal of the American Medical Association* found that narrow networks were associated with longer wait times for appointments, as in-network providers often face higher patient volumes. For a 65-year-old with diabetes, this delay could mean the difference between managing the condition effectively and facing complications like kidney failure or limb amputation.
To navigate narrow networks, patients must become proactive advocates for their own care. Start by scrutinizing your plan’s provider list before enrolling—don’t wait until you’re sick. If you have a pre-existing condition, contact your current specialists to confirm their in-network status. For those already enrolled, consider appealing out-of-network denials by demonstrating that in-network providers lack the necessary expertise. Finally, keep detailed records of all communications with your insurer; this documentation can be crucial if you need to escalate a dispute.
The takeaway is clear: narrow networks are a trade-off between affordability and access. While they may lower premiums, they shift risk onto patients, who must weigh the cost of limited choices against the potential for catastrophic expenses. As insurers continue to prioritize profits over patient care, consumers must stay informed, vigilant, and ready to fight for the healthcare they deserve.
Target's Medical Insurance: What's Covered and What's Not?
You may want to see also
Explore related products






![]()
High Deductibles: Steep out-of-pocket costs deter patients from seeking necessary medical care
High deductibles have become a formidable barrier to healthcare access, forcing patients to weigh their financial stability against their medical needs. Consider a 45-year-old with a family plan and a $5,000 deductible. When a persistent cough evolves into a potential pneumonia diagnosis, the out-of-pocket cost for a doctor’s visit, chest X-ray, and antibiotics could easily surpass $1,000 before insurance coverage kicks in. Faced with this expense, many delay or forgo care, risking complications that could have been prevented with early intervention. This scenario isn’t hypothetical—it’s a reality for millions, as studies show that 44% of Americans with high-deductible plans skip necessary care due to cost concerns.
The design of high-deductible plans shifts financial risk from insurers to consumers, often under the guise of encouraging "responsible healthcare spending." However, this approach fails to distinguish between discretionary care and essential treatment. For instance, a diabetic patient needing insulin or a cancer survivor requiring follow-up scans cannot afford to delay care, yet the upfront costs often force them to ration medication or skip appointments. Insurers argue that high deductibles lower premiums, but this trade-off is illusory for those who cannot absorb sudden, large expenses. The result? A system where financial vulnerability dictates health outcomes.
To navigate this landscape, patients must adopt strategic financial planning. First, maximize contributions to Health Savings Accounts (HSAs), which offer tax advantages and can offset out-of-pocket costs. Second, scrutinize insurance plans during open enrollment, focusing on deductible amounts and covered preventive services—some plans waive deductibles for annual checkups or screenings. Third, negotiate medical bills directly with providers; many hospitals offer discounts or payment plans for uninsured or underinsured patients. Finally, leverage generic medications and low-cost clinics for routine care, reducing reliance on expensive specialists.
Critics argue that high deductibles disproportionately harm low-income and chronically ill populations, exacerbating health disparities. A 2021 Commonwealth Fund study found that 38% of adults in high-deductible plans reported worsening health due to delayed care, compared to 27% in traditional plans. This trend underscores a systemic failure: insurance should mitigate risk, not create it. Policymakers must address this issue by capping out-of-pocket maximums, expanding subsidies, and mandating transparent pricing. Until then, patients must advocate for themselves, balancing financial prudence with the irreplaceable value of timely medical care.
Top Individual Health Insurance Plans: Finding the Best Coverage for You
You may want to see also
Explore related products






![]()
Claim Denials: Frequent rejections of valid claims force patients to fight for coverage
Health insurance companies often deny claims for reasons that seem trivial or opaque, leaving patients bewildered and financially burdened. For instance, a 2020 study found that nearly 20% of claims submitted to private insurers were initially denied, with many rejections stemming from administrative errors, such as missing documentation or coding discrepancies. These denials are not just inconveniences; they force patients to navigate a complex appeals process, often requiring multiple phone calls, resubmissions, and even legal intervention to secure coverage they’ve already paid for.
Consider the case of a 45-year-old patient prescribed a $1,200-per-month specialty medication for rheumatoid arthritis. Despite her doctor’s detailed justification, her insurer denied the claim, citing a lack of "medical necessity." This forced her to file an appeal, during which time she had to either pay out-of-pocket or forgo treatment, risking irreversible joint damage. Such scenarios highlight how claim denials not only delay care but also place undue emotional and financial strain on patients, particularly those with chronic conditions.
To combat this, patients must familiarize themselves with their policy’s coverage criteria and document every interaction with their insurer. For example, if a claim is denied for a high-cost procedure like an MRI, request a detailed explanation in writing and compare it against the policy’s terms. Keep a log of all communications, including dates, names, and outcomes, as this documentation can be crucial during an appeal. Additionally, leverage external resources like patient advocacy groups or state insurance commissioners, who can provide guidance and intervene on your behalf.
While insurers argue that denials help control costs and prevent fraud, the frequency and opacity of rejections suggest a systemic issue. A comparative analysis of Medicare and private insurers reveals that Medicare denies claims at a significantly lower rate, partly due to clearer guidelines and less financial incentive to reject claims. This disparity underscores the need for regulatory reforms that standardize claim review processes and penalize insurers for unjustified denials, ensuring patients aren’t forced to fight for coverage they’re entitled to.
Ultimately, the prevalence of claim denials reflects a broader imbalance of power between insurers and patients. By understanding their rights, meticulously documenting their efforts, and advocating for systemic change, patients can mitigate the impact of these denials. However, the onus should not fall solely on individuals; policymakers must address the root causes of this issue, ensuring that access to healthcare isn’t obstructed by profit-driven practices.
Insurance Premiums: Accident-Free but Still High?
You may want to see also
Explore related products





![]()
Complex Policies: Confusing terms and conditions make it hard for patients to understand benefits
Health insurance policies are often riddled with jargon and complex terms that leave patients perplexed. Imagine a 65-year-old retiree trying to decipher the difference between "out-of-pocket maximum" and "coinsurance" while selecting a Medicare Advantage plan. The confusion doesn’t just stem from unfamiliar words; it’s the lack of clarity on how these terms impact their actual healthcare costs. For instance, a policy might state a $3,000 out-of-pocket maximum but fail to explain that certain procedures or medications don’t count toward this limit. This opacity forces patients to make uninformed decisions, often leading to unexpected bills or underutilization of benefits.
Consider the process of comparing two health plans. Plan A offers 80% coverage for specialist visits after a $50 copay, while Plan B covers 100% after a $75 deductible. Which is better? Without a clear breakdown of how these terms translate into real-world costs, patients are left guessing. Insurance companies rarely provide tools like cost calculators or simplified summaries, leaving individuals to navigate a maze of fine print. This complexity disproportionately affects vulnerable populations, such as those with limited literacy or non-native English speakers, who may not have the resources to seek clarification.
The intentional use of convoluted language in policies serves a purpose: it shields insurance companies from scrutiny and reduces their financial liability. By making benefits difficult to understand, insurers can avoid overpaying claims and discourage policyholders from fully utilizing their coverage. For example, a patient might skip a necessary MRI because they incorrectly assume it’s not covered, saving the insurer thousands. This strategic ambiguity is a barrier to care, masquerading as a legal document.
To combat this, patients can take proactive steps. First, request a Summary of Benefits and Coverage (SBC) from their insurer, which provides a standardized overview of key terms. Second, use online resources like Healthcare.gov’s glossary to decode insurance jargon. Third, consult a broker or healthcare advocate who can explain policy details in plain language. For instance, understanding that "preauthorization" means getting insurer approval before a procedure can prevent claim denials. While these steps require effort, they empower patients to navigate complex policies and access the care they’re entitled to.
Ultimately, the onus should not be on patients to decipher their insurance. Policymakers must mandate clearer, more transparent policy language and hold insurers accountable for misleading practices. Until then, patients must arm themselves with knowledge and tools to unravel the complexities of their health insurance, ensuring they receive the benefits they pay for without unnecessary hurdles.
Medical IDs: Insurance and Your Health
You may want to see also
Frequently asked questions
Prior authorization is often required to control costs and ensure treatments are medically necessary. However, it can delay access to care, as providers must submit requests and wait for approval, sometimes leading to frustration for patients and providers alike.
Insurance companies may deny claims if they deem a treatment experimental, not medically necessary, or outside the scope of the policy. This practice helps manage costs but can make it harder for patients to access needed care, often requiring appeals or alternative solutions.
Insurance companies negotiate contracts with specific providers to keep costs down, creating narrower networks. While this reduces premiums, it can limit patient choice and make it harder to access specialists or providers in certain areas, particularly in rural or underserved regions.