The mandate to have health insurance, a key provision of the Affordable Care Act (ACA), required most Americans to obtain health coverage or pay a penalty, aiming to expand access to healthcare and reduce uninsured rates. However, in 2017, the Tax Cuts and Jobs Act effectively repealed this mandate by reducing the penalty to $0 starting in 2019, though the requirement itself technically remained on the books. This change sparked debates about its impact on insurance markets, with critics arguing it could lead to higher premiums and reduced coverage, while supporters viewed it as relief from a burdensome regulation. Despite the repeal of the penalty, the broader ACA framework remains in place, and the mandate’s legacy continues to influence discussions about healthcare policy in the United States.
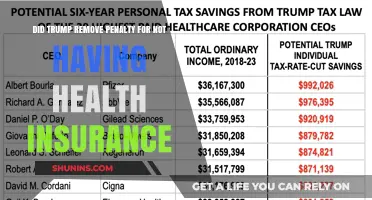
| Characteristics | Values |
|---|---|
| Mandate Type | Individual Mandate (part of the Affordable Care Act, ACA) |
| Original Implementation | 2010 (Affordable Care Act) |
| Effective Date | January 1, 2014 |
| Penalty for Non-Compliance | Tax penalty (calculated as a percentage of income or a flat fee, whichever was higher) |
| Repeal Status | The tax penalty for not having health insurance was effectively repealed starting January 1, 2019, via the Tax Cuts and Jobs Act of 2017. |
| Current Federal Mandate | No federal penalty for not having health insurance (as of 2023) |
| State-Level Mandates | Some states (e.g., California, Massachusetts, New Jersey, Rhode Island, Vermont) have implemented their own health insurance mandates with penalties for non-compliance. |
| Impact on ACA | The repeal of the federal mandate did not repeal the ACA itself; other provisions remain in effect, such as pre-existing condition protections and Medicaid expansion. |
| Public Opinion | Mixed; some support the repeal for reducing financial burden, while others argue it undermines the ACA's goal of universal coverage. |
| Coverage Impact | Studies indicate a slight decrease in health insurance coverage rates after the mandate repeal, particularly among younger and healthier individuals. |
| Legislative Efforts | No federal reinstatement of the mandate has been passed as of 2023, though some lawmakers continue to propose related policies. |
Explore related products






What You'll Learn
- ACA Individual Mandate Overview: Brief history and purpose of the Affordable Care Act's individual mandate
- Tax Penalty Elimination: How the Tax Cuts and Jobs Act removed the federal penalty in 2019
- State-Level Mandates: States like California and New Jersey that reinstated their own mandates
- Impact on Coverage Rates: Analysis of how repealing the mandate affected uninsured rates nationwide
- Political and Legal Debates: Ongoing discussions about reinstating or modifying the federal mandate
![]()
ACA Individual Mandate Overview: Brief history and purpose of the Affordable Care Act's individual mandate
The Affordable Care Act's (ACA) individual mandate, a cornerstone of healthcare reform, has undergone significant transformations since its inception. Enacted in 2010, the mandate required most Americans to obtain health insurance or face a tax penalty, aiming to expand coverage and reduce costs by broadening the risk pool. This provision took effect in 2014, marking a pivotal shift in U.S. healthcare policy. However, its journey has been marked by political and legal challenges, culminating in the repeal of the tax penalty in 2019, though the mandate itself remains on the books.
To understand the mandate’s purpose, consider the economic principle of adverse selection. Without a requirement to purchase insurance, healthier individuals might opt out, leaving insurers with a sicker, costlier population. The ACA’s mandate sought to counteract this by incentivizing broad participation, ensuring a balanced risk pool that could sustain lower premiums for all. For example, young, healthy adults—often less likely to purchase insurance—were critical to this equation. Their inclusion helped offset the costs of covering older, more vulnerable populations.
The mandate’s enforcement mechanism, a tax penalty for non-compliance, was a key point of contention. Initially set at $95 per adult or 1% of income in 2014, it escalated to $695 or 2.5% of income by 2016, whichever was higher. This financial incentive was designed to encourage compliance, but it also sparked debates about affordability and fairness. Critics argued that the penalty disproportionately affected lower-income individuals, while proponents highlighted the mandate’s role in stabilizing the insurance market.
In 2017, the Tax Cuts and Jobs Act effectively repealed the tax penalty, reducing it to $0 starting in 2019. This change raised questions about the mandate’s continued effectiveness. While the requirement to have insurance remains in law, the absence of a penalty has led some states to reintroduce their own mandates to maintain market stability. For instance, states like California and New Jersey have implemented state-level penalties for uninsured residents, underscoring the mandate’s enduring relevance in shaping healthcare policy.
Practically, the individual mandate’s history offers lessons for policymakers and consumers alike. For individuals, understanding the mandate’s purpose highlights the importance of continuous coverage, even in the absence of a federal penalty. For policymakers, it serves as a reminder of the delicate balance between incentivizing participation and ensuring affordability. As debates over healthcare reform continue, the ACA’s individual mandate remains a critical case study in the interplay between policy design and real-world outcomes.
Best Medical Insurance Company in Kenya: Who's Leading?
You may want to see also
Explore related products






![]()
Tax Penalty Elimination: How the Tax Cuts and Jobs Act removed the federal penalty in 2019
The Affordable Care Act's individual mandate, which required most Americans to have health insurance or pay a penalty, was a cornerstone of the law's efforts to expand coverage. However, the Tax Cuts and Jobs Act (TCJA) of 2017 effectively neutralized this mandate by reducing the penalty to $0 starting in 2019. This change marked a significant shift in federal policy, raising questions about its impact on insurance markets and individual behavior.
The Mechanism of Elimination
The TCJA didn't explicitly repeal the individual mandate. Instead, it employed a strategic reduction of the penalty to zero, effectively rendering it unenforceable. This approach avoided a direct confrontation with the mandate's legal framework while achieving the same practical outcome. Imagine a law requiring you to wear a seatbelt with a fine of $0 for non-compliance – the law technically exists, but there's no consequence for ignoring it.
This zeroing-out strategy had a profound effect. Without the financial penalty, the mandate lost its primary enforcement mechanism, essentially gutting its effectiveness.
Consequences and Considerations
The elimination of the penalty sparked debates about its potential consequences. Critics argued it would lead to a decline in insurance coverage as healthy individuals, no longer facing a financial disincentive, opted out of purchasing plans. This could result in a sicker risk pool, driving up premiums for those who remained insured. Proponents countered that the mandate was an unnecessary intrusion on individual liberty and that the market would adjust, potentially leading to more affordable, tailored insurance options.
Real-world data following the penalty's elimination showed a modest decline in insurance coverage, particularly among younger, healthier individuals. However, the predicted dramatic collapse of the insurance market didn't materialize, suggesting a more complex interplay of factors influencing coverage decisions.
Practical Implications for Individuals
For individuals, the elimination of the penalty meant greater flexibility in their healthcare choices. Those who felt healthy and financially secure could opt out of insurance without facing a tax penalty. However, this decision carried inherent risks. Unexpected illnesses or accidents could result in substantial out-of-pocket expenses. It's crucial to carefully weigh the potential savings against the financial vulnerability of being uninsured.
Consider factors like your age, health status, family history, and financial resources when making this decision. Consulting with a healthcare professional or insurance advisor can provide valuable guidance tailored to your specific circumstances.
Essential Steps to Verify Your Health Insurance Coverage Effectively
You may want to see also
Explore related products





![]()
State-Level Mandates: States like California and New Jersey that reinstated their own mandates
In the wake of the federal individual mandate's repeal in 2019, several states took matters into their own hands, crafting and reinstating health insurance mandates to ensure their residents remained covered. California and New Jersey emerged as pioneers in this movement, implementing state-level requirements that mirrored the erstwhile federal policy. California’s mandate, effective since 2020, imposes a penalty on uninsured residents unless they qualify for an exemption, such as financial hardship or religious beliefs. New Jersey followed suit in 2020, enacting a similar mandate with penalties tied to state tax returns. These actions reflect a broader trend of states asserting autonomy in healthcare policy, particularly in response to federal shifts.
Analyzing the impact of these mandates reveals both successes and challenges. California’s mandate, for instance, has contributed to a lower uninsured rate compared to the national average, demonstrating its effectiveness in closing coverage gaps. However, critics argue that penalties may burden low-income individuals who struggle to afford insurance despite subsidies. New Jersey’s approach includes robust outreach efforts to educate residents about available coverage options, which has helped mitigate confusion and increase enrollment. Both states’ experiences underscore the importance of pairing mandates with accessible, affordable insurance plans to maximize their benefits.
For states considering similar mandates, a step-by-step approach can enhance implementation. First, assess the existing uninsured population to identify gaps and tailor policies accordingly. Second, integrate mandates with expanded Medicaid or state-run marketplaces to ensure affordability. Third, allocate resources for public awareness campaigns to inform residents about their obligations and options. Cautions include avoiding overly punitive penalties that may alienate vulnerable populations and ensuring exemptions are clearly defined to prevent unintended consequences.
Comparatively, California and New Jersey’s mandates highlight the flexibility of state-level policymaking. While California’s penalty structure aligns closely with the former federal mandate, New Jersey’s emphasis on education and outreach offers a more proactive model. This diversity in approach allows other states to draw lessons based on their unique demographics and political landscapes. Ultimately, the success of these mandates hinges on balancing enforcement with accessibility, ensuring that the goal of universal coverage is achieved without undue hardship.
Practically, residents in these states should familiarize themselves with the specifics of their mandates to avoid penalties. In California, for example, the penalty for 2023 is calculated as either a flat fee of $800 per adult and $400 per child, or 2.5% of household income, whichever is higher. New Jersey’s penalty is slightly lower, set at $709 per adult and $354.50 per child. Both states offer exemptions for those facing financial hardships or other qualifying circumstances. Proactive steps, such as enrolling in coverage during open enrollment periods or exploring subsidy eligibility, can help individuals comply with the mandate while securing essential health benefits.
Life Insurance: Medication Lies and Their Impact
You may want to see also
Explore related products

$2.51 $2.99





![]()
Impact on Coverage Rates: Analysis of how repealing the mandate affected uninsured rates nationwide
The repeal of the individual mandate penalty in 2019 marked a significant shift in U.S. healthcare policy, eliminating the financial penalty for not having health insurance. This change was expected to influence coverage rates, but the extent of its impact required careful analysis. Initial projections suggested that millions could lose coverage as the mandate’s incentive to enroll was removed. However, the actual effects were nuanced, varying by state, demographic, and economic factors. Understanding these changes is critical for policymakers and individuals navigating the post-mandate healthcare landscape.
Analyzing the Data: Trends in Uninsured Rates Post-Repeal
Nationally, uninsured rates did rise following the repeal, but not as sharply as some predicted. From 2017 to 2021, the uninsured rate increased from 8.6% to 9.6%, according to Census Bureau data. States that expanded Medicaid under the Affordable Care Act (ACA) saw smaller increases compared to non-expansion states, highlighting the role of state-level policies in mitigating the impact. Younger, healthier individuals were more likely to drop coverage, as they faced fewer immediate health risks and no longer faced a penalty for being uninsured. This demographic shift had broader implications for risk pools, potentially increasing premiums for those who remained insured.
Economic and Policy Factors at Play
The repeal’s impact was not solely driven by the absence of a penalty. Economic factors, such as rising premiums and reduced federal funding for outreach, also contributed to declining coverage rates. For instance, the Trump administration cut funding for ACA navigators by 80% in 2017, making it harder for individuals to enroll in plans. Simultaneously, premium increases outpaced wage growth for many Americans, making insurance less affordable even without the mandate. These overlapping challenges suggest that the repeal was one of several factors eroding coverage gains achieved under the ACA.
Practical Implications for Individuals and Families
For those considering dropping coverage, it’s essential to weigh the risks. While healthy individuals may save on premiums in the short term, unexpected medical expenses can lead to financial strain. For example, a single emergency room visit can cost thousands of dollars, far exceeding the annual cost of a mid-tier insurance plan. Families with children or individuals with preexisting conditions should carefully evaluate alternatives, such as short-term health plans or Medicaid, though these options often come with limitations in coverage.
Policy Takeaways and Future Directions
The repeal of the mandate underscored the fragility of coverage gains tied to specific policy mechanisms. To stabilize uninsured rates, policymakers could explore alternatives such as auto-enrollment systems, state-level mandates, or enhanced subsidies for low-income individuals. For instance, states like New Jersey and California have implemented their own mandates, maintaining higher coverage rates than the national average. Such approaches demonstrate that while the federal mandate may be gone, innovative solutions can still protect access to healthcare.
TMJ and Retainers: Insurance Coverage Explained
You may want to see also
Explore related products






![]()
Political and Legal Debates: Ongoing discussions about reinstating or modifying the federal mandate
The Affordable Care Act's individual mandate, which required most Americans to have health insurance or pay a penalty, was effectively repealed in 2017 when Congress reduced the penalty to $0 as part of the Tax Cuts and Jobs Act. This change, implemented in 2019, sparked ongoing political and legal debates about whether to reinstate or modify the federal mandate. These discussions are deeply intertwined with broader conversations about healthcare accessibility, affordability, and the role of government in ensuring coverage.
Analytically, the repeal of the mandate has had measurable impacts on insurance markets. Without the penalty, healthier individuals were more likely to opt out of coverage, leading to riskier insurance pools and higher premiums for those who remained insured. This trend disproportionately affected younger and healthier demographics, who often viewed the cost of insurance as outweighing the benefits. Proponents of reinstating the mandate argue that it is essential for stabilizing the individual insurance market and ensuring broad risk-sharing, a principle critical to the ACA's framework. Critics, however, contend that forcing individuals to purchase insurance infringes on personal liberty and that alternatives, such as subsidies or auto-enrollment policies, could achieve similar goals without coercion.
Instructively, policymakers considering reinstating or modifying the mandate must weigh several practical factors. First, they should assess the penalty amount: a nominal fee might be insufficient to incentivize enrollment, while a steep penalty could provoke public backlash. Second, any mandate must be paired with affordability measures, such as expanding premium tax credits or capping out-of-pocket costs, to ensure compliance without causing financial hardship. Third, policymakers could explore hybrid models, such as a mandate with exemptions for low-income individuals or those in states with high insurance costs, to balance equity and feasibility.
Persuasively, the debate over the mandate reflects deeper ideological divides in American politics. Progressives often frame the mandate as a necessary tool for achieving universal coverage, emphasizing collective responsibility for health outcomes. Conservatives, meanwhile, view it as an overreach of federal power, advocating instead for market-based solutions and individual choice. These perspectives are not mutually exclusive, however. A modified mandate, for instance, could incorporate conservative principles by allowing states greater flexibility in designing their own coverage requirements while maintaining a federal floor to prevent "race-to-the-bottom" dynamics.
Comparatively, international examples offer insights into alternative approaches. Countries like Switzerland and the Netherlands employ mandates but couple them with robust subsidies and regulated insurance markets, ensuring affordability and accessibility. In contrast, nations without mandates, such as Canada, rely on single-payer systems to achieve near-universal coverage. These models suggest that while mandates can be effective, their success depends on complementary policies that address cost and availability. U.S. policymakers could draw lessons from these examples by crafting a mandate that aligns with the nation’s mixed public-private healthcare system.
Descriptively, the current landscape of mandate discussions is characterized by partisan gridlock and incremental state-level actions. In the absence of federal action, some states have implemented their own mandates or penalties for lacking coverage, while others have actively resisted such measures. This patchwork approach underscores the complexity of reinstating a federal mandate in a politically polarized environment. Moving forward, any federal proposal will need to navigate these divisions, potentially by framing the mandate as a tool for market stability rather than a partisan policy goal. Practical tips for stakeholders include engaging in bipartisan dialogue, leveraging data to demonstrate the mandate’s impact, and exploring phased implementation to build public support.
Medical Expense Insurance: Financial Safety Net for Health Emergencies
You may want to see also
Frequently asked questions
Yes, the individual mandate penalty under the Affordable Care Act (ACA) was effectively repealed starting in 2019 as part of the Tax Cuts and Jobs Act of 2017.
No, the repeal only eliminated the federal penalty for not having health insurance. Some states have implemented their own mandates and penalties, so it’s important to check your state’s requirements.
Yes, you can still enroll in health insurance through the ACA marketplace, private insurers, or employer-sponsored plans. The repeal of the mandate did not affect the availability of coverage options.