The issue of uninsured Americans remains a pressing concern in the United States, with millions of citizens lacking access to adequate health coverage. Despite efforts to expand healthcare access, a significant portion of the population continues to face barriers to obtaining insurance, whether due to high costs, limited availability, or other socioeconomic factors. Understanding the scope of this problem is crucial, as it not only impacts individual health outcomes but also places a substantial burden on the broader healthcare system and economy. Recent data highlights the disparities in coverage, shedding light on the demographic groups most affected and the underlying reasons behind the persistence of this issue in one of the world’s wealthiest nations.
| Characteristics | Values |
|---|---|
| Total Uninsured Americans (2022) | Approximately 28.9 million (8.5% of the population) |
| Age Group with Highest Uninsured | Young adults (18-24 years old) |
| Uninsured Rate by Race/Ethnicity | Hispanic (19.1%), American Indian/Alaska Native (16.9%), Black (9.9%) |
| Uninsured Rate by Income Level | Lowest income group (below 138% of poverty level) |
| Uninsured Rate by State | Texas (18.4%), Oklahoma (14.3%), Georgia (13.4%) (highest rates) |
| Uninsured Rate by Employment Status | Part-time workers and self-employed individuals |
| Uninsured Rate by Education Level | Adults with less than a high school education |
| Uninsured Children (2022) | Approximately 4.3 million (5.6% of children) |
| Impact of Affordable Care Act (ACA) | Reduced uninsured rate from 16% in 2010 to 8.5% in 2022 |
| Reasons for Being Uninsured | High cost of insurance, lack of employer-sponsored coverage, ineligibility for Medicaid |
Explore related products






What You'll Learn
![]()
Uninsured rates by state
The uninsured rate in the United States varies significantly by state, reflecting disparities in healthcare access, policy decisions, and socioeconomic factors. As of recent data, states like Texas and Florida consistently report higher uninsured rates, often exceeding 15% of their populations. In contrast, states such as Massachusetts and Vermont boast rates below 5%, largely due to their expansive Medicaid programs and state-level health insurance mandates. These variations highlight the critical role of state-level policies in shaping healthcare coverage.
Analyzing the data reveals a clear correlation between state policies and uninsured rates. States that have expanded Medicaid under the Affordable Care Act (ACA) tend to have lower uninsured rates, as this expansion extends coverage to low-income adults who previously fell into the "coverage gap." For instance, Kentucky, which expanded Medicaid in 2014, saw its uninsured rate drop from 14.3% to 5.5% by 2020. Conversely, states like Texas and Georgia, which have not expanded Medicaid, continue to struggle with higher uninsured rates, particularly among working-age adults.
Geographic and demographic factors also play a significant role in uninsured rates by state. Southern states, for example, often have higher uninsured rates due to a combination of lower median incomes, fewer employer-sponsored insurance options, and a higher proportion of workers in industries like agriculture and service, which typically offer fewer benefits. Additionally, states with large rural populations face unique challenges, such as limited access to healthcare providers and higher out-of-pocket costs, which can deter individuals from seeking coverage.
To address these disparities, policymakers and advocates must focus on tailored solutions. States with high uninsured rates could consider implementing state-level subsidies or reinsurance programs to make coverage more affordable. Public awareness campaigns can also help educate residents about available options, such as ACA marketplace plans or Medicaid enrollment. For individuals in states with limited coverage options, exploring alternatives like short-term health plans or health-sharing ministries may provide temporary relief, though these options often come with significant limitations.
Ultimately, understanding uninsured rates by state is crucial for identifying gaps in coverage and implementing effective solutions. While federal policies provide a framework, state-level actions are often the determining factor in ensuring access to healthcare. By examining these trends and taking proactive steps, states can work toward reducing uninsured rates and improving health outcomes for their residents.
Understanding Straight Medicare Insurance: The Basics
You may want to see also
Explore related products






![]()
Impact of income on coverage
Income is a critical determinant of health insurance coverage in the United States, with disparities starkly evident across economic strata. According to the U.S. Census Bureau, in 2022, 8.5% of Americans were uninsured, but this figure masks significant variation by income level. Among households earning below the federal poverty level (FPL), the uninsured rate was nearly 20%, compared to just 4.5% for those earning 400% above the FPL or more. This gap underscores how financial constraints directly limit access to health coverage, even with programs like Medicaid and the Affordable Care Act (ACA) subsidies in place.
Consider the mechanics of this disparity: lower-income individuals often face a Catch-22. While Medicaid is designed to cover those below 138% of the FPL, not all states have expanded Medicaid under the ACA, leaving millions in the "coverage gap"—earning too much for Medicaid but too little for ACA subsidies. For instance, in Texas, which has not expanded Medicaid, an estimated 1.5 million residents fall into this gap, unable to afford private insurance despite their income slightly exceeding Medicaid eligibility. This highlights how geographic and policy factors compound income-based disparities.
A persuasive argument emerges when examining the long-term consequences of income-driven coverage gaps. Uninsured individuals are more likely to delay or forgo necessary care, leading to worse health outcomes and higher costs when conditions become acute. For example, a study in *Health Affairs* found that uninsured adults are 25% more likely to die prematurely than their insured counterparts. This not only affects individual well-being but also strains the healthcare system, as untreated conditions often result in costly emergency room visits. Closing income-based coverage gaps is thus not just a moral imperative but an economic one.
To address this issue, practical steps can be taken. First, states should expand Medicaid to cover more low-income residents, as evidenced by the success of expansion states like Kentucky, where uninsured rates dropped by over 50% post-expansion. Second, policymakers could enhance ACA subsidies to make marketplace plans more affordable for those just above the Medicaid threshold. For individuals, understanding eligibility criteria and enrollment periods is crucial; resources like Healthcare.gov provide tools to estimate costs and apply for subsidies. Finally, employers can play a role by offering more affordable health plans, particularly for low-wage workers, who are disproportionately uninsured.
In conclusion, the impact of income on health insurance coverage is profound and multifaceted, shaped by policy, geography, and individual circumstances. By targeting income-based disparities through systemic changes and informed decision-making, millions more Americans could gain access to the care they need. This is not merely a matter of statistics but of ensuring equitable health outcomes for all.
Understanding Social Security Medical Insurance Costs and Coverage
You may want to see also
Explore related products






![]()
Racial disparities in insurance
According to recent data, approximately 8.5% of Americans, or around 28 million people, lack health insurance. However, this figure masks significant racial disparities that persist in the U.S. healthcare system. For instance, while 5.4% of non-Hispanic white individuals are uninsured, the rates are substantially higher for other racial and ethnic groups: 9.3% of Black Americans, 19.1% of Hispanic Americans, and 8.3% of Asian Americans remain without coverage. These disparities are not merely numbers but reflect deeper systemic inequalities that affect access to care, health outcomes, and overall well-being.
To understand these disparities, consider the intersection of race with socioeconomic factors. Hispanic Americans, for example, are more likely to work in low-wage jobs that do not offer employer-sponsored insurance, a primary source of coverage for most Americans. Additionally, undocumented immigrants, who are disproportionately Hispanic, are ineligible for Medicaid or Affordable Care Act (ACA) marketplace plans, further limiting their access. Similarly, Black Americans face barriers such as higher rates of poverty and residential segregation, which often correlate with limited access to healthcare facilities and insurance providers. Addressing these disparities requires targeted policies that account for these unique challenges.
A comparative analysis reveals that states with higher uninsured rates among racial minorities often have stricter Medicaid eligibility criteria or have not expanded Medicaid under the ACA. For example, in Texas, where 18% of Hispanic residents are uninsured, the state has not expanded Medicaid, leaving many low-income individuals in the "coverage gap"—earning too much to qualify for Medicaid but too little to afford private insurance. In contrast, states like California, which expanded Medicaid and implemented outreach programs targeting diverse communities, have seen significant reductions in uninsured rates across racial groups. This highlights the importance of policy decisions in mitigating racial disparities in insurance coverage.
Practical steps can be taken to reduce these disparities. First, expanding Medicaid in all states would provide coverage to millions of low-income individuals, particularly in communities of color. Second, increasing funding for community health centers in underserved areas can improve access to care for uninsured populations. Third, culturally competent outreach programs can help educate diverse communities about available insurance options and enrollment processes. For example, bilingual navigators have been effective in assisting Hispanic populations with ACA enrollment. Finally, addressing systemic racism in healthcare and employment policies is essential to creating equitable access to insurance and care.
In conclusion, racial disparities in insurance coverage are a stark reminder of the persistent inequalities in the U.S. healthcare system. By focusing on policy changes, targeted interventions, and systemic reforms, it is possible to reduce these disparities and move toward a more equitable healthcare landscape. The data is clear: the uninsured rate is not just a number but a reflection of deeper social and economic injustices that demand urgent attention.
Getting Medical Insurance in the USA: A Step-by-Step Guide
You may want to see also
Explore related products





![]()
Effect of employment status
Employment status is a critical determinant of health insurance coverage in the United States, with profound implications for access to healthcare. As of recent data, approximately 8.6% of Americans, or roughly 28 million people, lack health insurance. Among these, a disproportionate number are either unemployed, working part-time, or employed in jobs that do not offer health benefits. For instance, in 2022, the uninsured rate for unemployed individuals was 19.5%, compared to just 7.3% for full-time workers. This stark disparity underscores the direct link between job stability and healthcare access.
Consider the mechanics of employer-sponsored insurance (ESI), which covers about 55% of the U.S. population. Full-time employees are more likely to receive ESI as part of their benefits package, while part-time or gig workers often fall through the cracks. For example, a 35-year-old working 20 hours a week at a retail job is unlikely to qualify for employer-provided insurance, leaving them to navigate the complexities of the individual market or rely on public programs like Medicaid. However, eligibility for Medicaid varies by state, and not all low-income individuals qualify, creating a coverage gap.
To mitigate the impact of employment status on insurance coverage, practical steps can be taken. First, individuals in part-time or gig roles should explore the Health Insurance Marketplace, where subsidies may reduce premiums based on income. For example, a single individual earning $30,000 annually might qualify for a premium tax credit, lowering monthly costs significantly. Second, states that have expanded Medicaid under the Affordable Care Act (ACA) offer coverage to adults earning up to 138% of the federal poverty level, a lifeline for those in low-wage jobs. Checking state-specific eligibility criteria is essential.
A comparative analysis reveals that countries with universal healthcare systems, such as Canada or the UK, do not face the same employment-insurance nexus. In contrast, the U.S. system ties coverage to jobs, leaving workers vulnerable during periods of unemployment or underemployment. This structural flaw was exacerbated during the COVID-19 pandemic, when millions lost jobs—and insurance—simultaneously. Policymakers could address this by decoupling insurance from employment, as proposed in single-payer models, or by expanding Medicaid nationwide to cover more low-income workers.
In conclusion, employment status is a pivotal factor in the uninsured rate among Americans, with part-time, gig, and unemployed individuals bearing the brunt of the coverage gap. By understanding the mechanics of ESI, exploring marketplace subsidies, and advocating for systemic reforms, individuals and policymakers can work toward reducing disparities. Until then, the link between job stability and healthcare access will remain a pressing issue, affecting millions of lives.
Are Psychiatrists Recognized as Specialists for Health Insurance Coverage?
You may want to see also
Explore related products

![]()
Role of policy changes
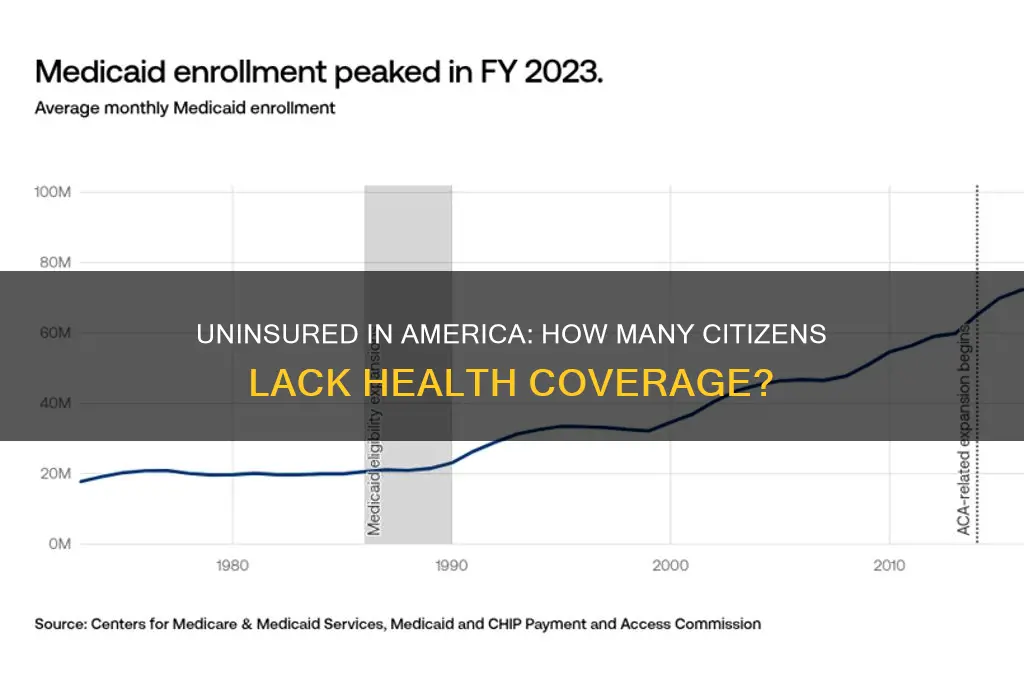
As of 2023, approximately 8% of Americans, or around 28 million people, lack health insurance, according to the U.S. Census Bureau. This figure fluctuates based on economic conditions, policy shifts, and demographic changes. Policy changes have historically been the most direct lever in reducing or increasing these numbers, often with immediate and measurable impacts. For instance, the Affordable Care Act (ACA) of 2010 cut the uninsured rate from 16% in 2010 to 8.6% by 2016, demonstrating the power of legislative action. Conversely, efforts to repeal or undermine the ACA have led to incremental increases in uninsured rates, particularly among low-income and marginalized populations.
Analyzing the ACA’s Medicaid expansion provides a clear example of policy impact. States that expanded Medicaid saw uninsured rates drop by an average of 10 percentage points more than non-expansion states. For example, Kentucky’s uninsured rate fell from 14.3% in 2013 to 5.8% in 2016 after expanding Medicaid. However, states like Texas and Florida, which opted out, continue to have uninsured rates above the national average, at 18% and 13%, respectively. This disparity underscores how policy decisions at the state level can either amplify or mitigate federal initiatives, creating a patchwork of access across the country.
Instructively, policymakers aiming to reduce uninsured rates should focus on three key areas: expanding eligibility, simplifying enrollment processes, and stabilizing insurance markets. For instance, automatically enrolling eligible individuals in Medicaid or ACA plans, as some states have piloted, can reduce barriers to access. Additionally, restoring funding for ACA navigators, which assist with enrollment, could increase sign-ups by up to 20%, based on pre-2017 data. Stabilizing markets involves capping out-of-pocket costs and reinstating cost-sharing reduction payments, which encourage insurers to offer affordable plans.
Persuasively, the moral and economic arguments for policy-driven insurance expansion are compelling. Uninsured individuals are more likely to delay care, leading to costlier emergency treatments and poorer health outcomes. A 2021 study found that uninsured adults were twice as likely to skip needed care due to cost. Economically, expanding coverage reduces uncompensated care costs for hospitals, which totaled $42 billion in 2020. By investing in policies that increase coverage, lawmakers can improve public health while alleviating financial strain on healthcare systems.
Comparatively, the U.S. lags behind peer nations in health insurance coverage due to its reliance on employer-based insurance and fragmented policy approach. Countries with universal healthcare, like Canada and the UK, maintain uninsured rates below 1%. Even nations with mixed systems, such as Germany, achieve near-universal coverage through mandatory insurance and government subsidies. The U.S. could adopt elements of these models, such as a public option or auto-enrollment systems, to close its coverage gap. However, political polarization remains a significant barrier to such reforms.
Descriptively, the landscape of uninsured Americans is diverse, with disparities along racial, geographic, and age lines. Non-elderly Black and Hispanic individuals are twice as likely as whites to be uninsured, while rural residents face higher rates due to limited provider networks and lower Medicaid expansion. Young adults aged 19–34, often caught in the gap between parental coverage and employer-based plans, represent a disproportionate share of the uninsured. Tailored policies, such as extending dependent coverage to age 26 (a provision of the ACA) or creating rural health subsidies, can address these specific vulnerabilities.
Applying for Medicare in South Carolina: A Guide
You may want to see also
Frequently asked questions
As of 2023, approximately 8% of the U.S. population, or around 27 million people, do not have health insurance.
The main reasons include high insurance costs, lack of employer-sponsored coverage, ineligibility for public programs like Medicaid, and gaps in coverage options.
Low-income individuals, young adults, people of color, and those living in states that did not expand Medicaid are disproportionately uninsured.
The uninsured rate has fluctuated, with a significant drop after the Affordable Care Act (ACA) was implemented in 2014, but it has risen slightly in recent years due to factors like policy changes and economic shifts.
Efforts include expanding Medicaid in more states, enhancing Affordable Care Act subsidies, promoting enrollment in public programs, and advocating for policy reforms to make coverage more affordable and accessible.