The issue of uninsured Americans remains a critical concern in the United States, reflecting broader challenges within the healthcare system. Despite efforts to expand coverage, millions of individuals still lack health insurance, leaving them vulnerable to financial hardship and limited access to medical care. Factors such as high insurance costs, employment status, and gaps in public programs contribute to this persistent problem. Understanding the scope and implications of this issue is essential for addressing disparities and improving overall health outcomes in the nation.
Explore related products

$14.77 $18





What You'll Learn
![]()
Uninsured rates by state
Texas leads the nation in uninsured rates, with approximately 18% of its residents lacking health coverage. This stark figure is nearly double the national average, highlighting significant disparities in access to healthcare. The state’s decision not to expand Medicaid under the Affordable Care Act (ACA) plays a critical role, leaving many low-income adults in a coverage gap—earning too much for traditional Medicaid but too little for ACA subsidies. High uninsured rates in Texas also correlate with its large population of undocumented immigrants, who are ineligible for most public insurance programs. Employers in the state are less likely to offer health benefits compared to national averages, further exacerbating the issue. Addressing this crisis requires policy changes, such as Medicaid expansion, to close the gap and improve health outcomes for millions.
In contrast, states like Massachusetts and Vermont boast uninsured rates below 3%, setting a benchmark for universal coverage. Massachusetts, often called the pioneer of health reform, implemented a state-level individual mandate in 2006, which later inspired the ACA. Its Connector program offers subsidized plans for low- and middle-income residents, while robust employer-sponsored insurance and Medicaid expansion ensure broad access. Vermont’s success stems from its commitment to a single-payer system, though it has not fully materialized, and its focus on expanding Medicaid and creating a state-run marketplace. These states demonstrate that a combination of policy innovation, public investment, and political will can achieve near-universal coverage, even in a diverse national landscape.
Southern states dominate the list of highest uninsured rates, with Georgia (12.9%), Florida (12.8%), and Mississippi (12.7%) trailing closely behind Texas. This regional trend is tied to shared policy decisions, such as rejecting Medicaid expansion, which leaves millions of working-poor adults without affordable options. The South also faces unique challenges, including lower median incomes, higher poverty rates, and a larger proportion of small businesses that do not provide health benefits. Cultural and political resistance to federal healthcare programs further compounds the issue. Targeted outreach, simplified enrollment processes, and state-specific solutions could help mitigate these disparities, but progress remains slow in the absence of broader policy shifts.
For individuals in high-uninsured states, understanding available resources is crucial. In non-expansion states, residents earning below 100% of the federal poverty level ($13,590 for an individual in 2023) are generally ineligible for subsidies but also do not qualify for Medicaid, creating a "coverage gap." Those slightly above this threshold can explore ACA marketplace plans, where subsidies may significantly reduce costs. Community health centers offer sliding-scale fees for uninsured patients, providing essential care regardless of ability to pay. Additionally, short-term health plans, while limited in coverage, can serve as a temporary bridge for those between jobs or awaiting eligibility for other programs. Knowing these options empowers individuals to navigate a fragmented system and secure necessary care.
Finally, the variation in uninsured rates by state underscores the need for localized solutions within a national framework. While federal policies like the ACA have reduced uninsured rates overall, state-level decisions—such as Medicaid expansion and marketplace investments—determine success on the ground. States with lower uninsured rates provide models for others, but replication requires tailoring to regional demographics, economies, and political climates. Advocacy for uniform coverage standards must be paired with flexibility to address unique challenges. Until then, the patchwork of access will persist, leaving millions vulnerable in states where systemic barriers remain unaddressed.
Life and Health Insurance Exam: PA's Challenge
You may want to see also
Explore related products






![]()
Impact of income on coverage
Income is a decisive factor in determining whether Americans have health insurance, with lower-income individuals facing significantly higher uninsured rates. According to the U.S. Census Bureau, in 2022, 8.0% of Americans lacked health insurance, but this figure masks stark disparities: 13.3% of those living below the federal poverty level were uninsured, compared to just 4.8% of those with incomes at or above 400% of the poverty level. This gap underscores how financial constraints directly limit access to coverage.
Consider the mechanics of this disparity. For low-income families, even subsidized plans under the Affordable Care Act (ACA) can be unaffordable. Premiums, deductibles, and copays often consume a disproportionate share of their budget. For example, a family of four earning $30,000 annually might face a benchmark plan premium of $200/month, plus a $3,000 deductible—an insurmountable expense when rent, food, and utilities already stretch their income. In contrast, higher-income households can more easily absorb these costs, making coverage a practical choice rather than a financial gamble.
The impact of income on coverage also varies by state, particularly in those that have not expanded Medicaid under the ACA. In these states, individuals earning too much for traditional Medicaid but too little for ACA subsidies fall into the "coverage gap." For instance, in Texas, an estimated 1.2 million residents earn too much to qualify for Medicaid but cannot afford private insurance. This gap disproportionately affects workers in low-wage industries like retail and hospitality, where employer-sponsored insurance is rare or inadequate.
To mitigate these disparities, policymakers and advocates should focus on targeted solutions. Expanding Medicaid in all states would immediately reduce uninsured rates among low-income adults. Additionally, increasing subsidy eligibility and capping premium contributions as a percentage of income could make coverage more accessible. For example, capping premiums at 5% of income for those earning below 200% of the poverty level could reduce financial barriers for millions. Practical steps like these would address the root cause of income-based coverage gaps, ensuring that financial status does not dictate access to healthcare.
Driving Less: How Reduced Mileage Impacts Your Car Insurance Rates
You may want to see also
Explore related products






![]()
Racial disparities in insurance
According to recent data, approximately 8.5% of Americans, or around 28 million people, were uninsured in 2021. However, this figure masks significant racial disparities in insurance coverage. For instance, while 5.4% of non-Hispanic whites lacked insurance, the rates were substantially higher for other racial groups: 9.3% of Blacks, 18.3% of Hispanics, and 6.7% of Asians were uninsured. These disparities highlight systemic inequalities in access to healthcare, which are deeply rooted in socioeconomic and historical factors.
To understand these disparities, consider the intersection of race and income. Hispanics, for example, are more likely to work in low-wage jobs that do not offer employer-sponsored insurance, a primary source of coverage for most Americans. Additionally, undocumented immigrants, who are disproportionately Hispanic, are ineligible for Medicaid or Affordable Care Act (ACA) marketplace plans, further limiting their options. For Blacks, historical redlining and systemic racism have led to generational wealth gaps, reducing their ability to afford private insurance. Addressing these disparities requires targeted policies, such as expanding Medicaid in states that have not yet done so, which would disproportionately benefit communities of color.
A comparative analysis reveals that states with higher uninsured rates among minorities often have stricter eligibility criteria for Medicaid. For example, in Texas, where 18% of Hispanics are uninsured, the state has not expanded Medicaid under the ACA, leaving many low-income individuals without coverage. In contrast, states like California, which expanded Medicaid and implemented robust outreach programs, have significantly lower uninsured rates among racial minorities. This suggests that policy decisions at the state level play a critical role in exacerbating or mitigating racial disparities in insurance coverage.
Practical steps can be taken to reduce these disparities. First, increasing funding for community health centers in underserved areas can provide a safety net for uninsured individuals. Second, multilingual outreach campaigns can improve awareness of available insurance options among non-English-speaking populations. Third, advocating for federal policies that decouple immigration status from eligibility for healthcare coverage could address the unique challenges faced by undocumented individuals. By implementing these measures, we can move toward a more equitable healthcare system that ensures coverage for all Americans, regardless of race.
Finally, it is essential to recognize that racial disparities in insurance are not merely a healthcare issue but a reflection of broader societal inequalities. For instance, Blacks and Hispanics are more likely to live in areas with limited access to healthcare providers, compounding their challenges in obtaining insurance and care. Addressing these disparities requires a multifaceted approach that includes not only healthcare reform but also efforts to tackle housing discrimination, educational inequities, and economic inequality. Only by addressing these root causes can we hope to achieve meaningful progress in reducing racial disparities in insurance coverage.
Gap Life Insurance: What You Need to Know
You may want to see also
Explore related products





![]()
Effect of policy changes
Policy changes have a direct and measurable impact on the number of uninsured Americans, often shifting the landscape of healthcare access within months of implementation. For instance, the Affordable Care Act (ACA) of 2010 led to a significant reduction in the uninsured rate, dropping from 16% in 2010 to 8.6% in 2016. This was achieved through expansions in Medicaid eligibility, the creation of health insurance marketplaces, and subsidies for low- to middle-income individuals. Conversely, policy rollbacks or reductions in funding, such as the elimination of the individual mandate penalty in 2019, have been linked to increases in uninsured rates, particularly among younger and healthier populations who may forgo coverage without a financial incentive.
To understand the effect of policy changes, consider the role of Medicaid expansion as a case study. States that expanded Medicaid under the ACA saw uninsured rates drop by an average of 10 percentage points more than non-expansion states. For example, Kentucky’s uninsured rate fell from 14.3% in 2013 to 5.8% in 2016 after expanding Medicaid. However, states like Texas and Florida, which did not expand Medicaid, experienced slower declines and higher uninsured rates, particularly among low-income adults. This disparity highlights how state-level decisions, influenced by federal policy frameworks, can create vastly different outcomes for residents.
When crafting or evaluating policy changes, it’s crucial to consider unintended consequences. For example, while the ACA aimed to increase coverage, some individuals faced higher premiums or limited provider networks, leading to dissatisfaction. Similarly, policies targeting specific age groups, such as allowing young adults to stay on parental insurance until age 26, successfully reduced uninsured rates among 18- to 25-year-olds by 10%. However, such targeted policies may leave gaps for other demographics, such as undocumented immigrants or those in the "coverage gap" earning too much for Medicaid but too little for subsidies. Policymakers must balance broad accessibility with tailored solutions to avoid exacerbating disparities.
A persuasive argument for proactive policy change lies in the economic and societal benefits of reducing uninsured rates. Uninsured individuals often delay care, leading to costlier emergency treatments and poorer health outcomes. For instance, states with lower uninsured rates report fewer preventable hospitalizations, saving billions in healthcare costs annually. By investing in policies that expand coverage—such as reinstating the individual mandate or further subsidizing marketplace plans—policymakers can reduce long-term healthcare expenditures while improving public health. The evidence is clear: strategic policy changes are not just moral imperatives but fiscally responsible decisions.
Finally, a comparative analysis of international policies offers valuable insights. Countries with universal healthcare systems, like Canada or the UK, maintain uninsured rates near 0%, while the U.S. hovers around 8-9%. While direct replication of these models may not be feasible, incremental policy changes inspired by such systems—such as a public option or automatic enrollment—could further reduce uninsured rates. For example, a public option could provide affordable coverage to those in states without Medicaid expansion, while automatic enrollment could simplify access for eligible individuals. By learning from global examples and adapting them to the U.S. context, policymakers can design more effective solutions to close the coverage gap.
Whole Life Insurance: Can You Collect Early?
You may want to see also
Explore related products



![]()
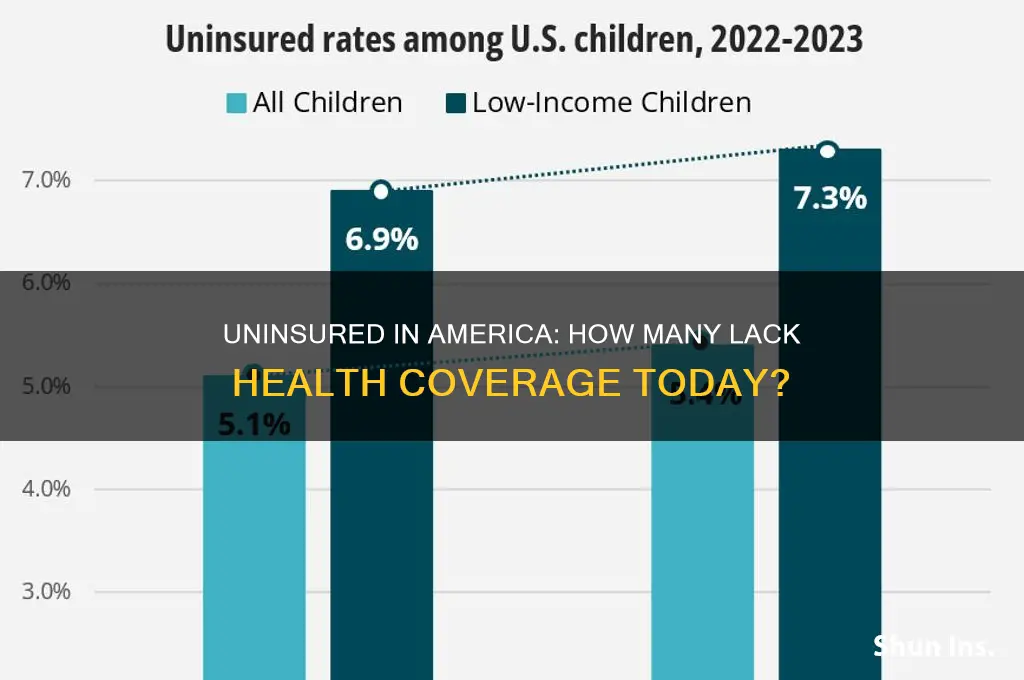
Uninsured children statistics
As of the latest data, approximately 4.3 million children in the United States lack health insurance, a figure that underscores a persistent gap in coverage despite broader trends of improvement. This statistic is particularly alarming when considering the long-term health and developmental consequences for uninsured children. Without access to preventive care, routine check-ups, and timely treatment, these children face higher risks of chronic conditions, delayed developmental milestones, and reduced overall well-being. The disparity in coverage often correlates with socioeconomic factors, with children in low-income families or those living in states that have not expanded Medicaid being disproportionately affected.
Analyzing the data reveals a stark divide in uninsured rates among children across different states. For instance, Texas leads the nation with over 800,000 uninsured children, accounting for nearly 20% of the national total. In contrast, states like Massachusetts and Vermont boast uninsured rates below 2%, thanks to robust state-level policies and expanded Medicaid programs. This variation highlights the critical role of state-level decisions in shaping children’s access to healthcare. Policymakers in states with high uninsured rates could look to successful models in other states to implement targeted solutions, such as simplifying enrollment processes or increasing funding for children’s health programs.
From a practical standpoint, addressing the issue of uninsured children requires a multi-faceted approach. Parents and caregivers can take proactive steps by exploring programs like the Children’s Health Insurance Program (CHIP), which provides low-cost coverage for children in families who earn too much to qualify for Medicaid but cannot afford private insurance. Additionally, schools and community organizations can play a vital role by hosting enrollment drives and educating families about available resources. For example, distributing bilingual materials and offering assistance with applications can help overcome barriers like language and complexity that often deter eligible families from enrolling.
A comparative analysis of uninsured children statistics also reveals racial and ethnic disparities. Hispanic children, for instance, are twice as likely to be uninsured as their non-Hispanic white peers, largely due to factors like immigration status and limited access to employer-sponsored insurance. Addressing these disparities requires culturally sensitive strategies, such as partnering with community leaders to build trust and ensuring that enrollment processes are inclusive of non-English speakers. By tackling these systemic barriers, we can move closer to the goal of universal coverage for children.
Finally, the moral and economic imperatives for insuring all children cannot be overstated. Uninsured children are more likely to end up in emergency rooms for treatable conditions, driving up healthcare costs for everyone. Moreover, investing in children’s health yields long-term benefits, including better educational outcomes, higher productivity, and reduced reliance on public assistance programs. As such, reducing the number of uninsured children is not just a matter of compassion but also a strategic investment in the nation’s future. Policymakers, healthcare providers, and communities must collaborate to close this coverage gap and ensure that every child has the opportunity to thrive.
Protect Your Luxury: A Guide to Insuring Designer Handbags
You may want to see also
Frequently asked questions
As of 2023, approximately 8% of Americans, or around 27 million people, are uninsured, according to the U.S. Census Bureau.
Young adults, low-income individuals, and people of color, particularly Hispanic and Native American populations, are disproportionately uninsured due to factors like cost, employment status, and access to coverage options.
The uninsured rate has fluctuated, with a significant decrease after the Affordable Care Act (ACA) was implemented in 2010, but it has risen slightly in recent years due to factors like policy changes and economic shifts.
The primary reasons include high insurance costs, lack of employer-sponsored coverage, ineligibility for public programs like Medicaid, and gaps in ACA coverage options in certain states.
The U.S. has a significantly higher uninsured rate compared to other developed nations, which typically have universal healthcare systems or broader public coverage options.