The disparity in health insurance coverage between Black and White populations in the United States remains a critical issue, reflecting broader systemic inequalities in healthcare access. While significant strides have been made in recent years to reduce the uninsured rate overall, data consistently shows that Black individuals are more likely to be uninsured compared to their White counterparts. Factors such as socioeconomic status, employment opportunities, and geographic location play a significant role in these disparities. Understanding these differences is essential for policymakers and healthcare providers to address the root causes and ensure equitable access to healthcare for all communities.
Explore related products






What You'll Learn
- Racial disparities in health insurance coverage rates across different states and regions
- Impact of income levels on health insurance access for Black and White populations
- Role of employer-based insurance in coverage gaps between racial groups
- Medicaid and Medicare enrollment differences among Black and White individuals
- Effects of healthcare policies on insurance disparities between Black and White communities
![]()
Racial disparities in health insurance coverage rates across different states and regions
Racial disparities in health insurance coverage persist across the United States, with Black individuals consistently experiencing lower rates of coverage compared to their White counterparts. Data from the U.S. Census Bureau reveals that in 2022, 9.1% of Black people were uninsured, compared to 5.9% of White people. This gap, though narrowing over the past decade, remains significant and varies widely by state and region. Southern states, such as Texas, Georgia, and Mississippi, exhibit some of the largest disparities, where both higher uninsured rates overall and more pronounced racial gaps are observed. For instance, in Texas, 17.7% of Black individuals lacked insurance in 2022, compared to 12.8% of White individuals, highlighting systemic barriers to access in these regions.
To understand these disparities, it’s essential to examine the interplay of state policies, economic factors, and historical inequities. States that expanded Medicaid under the Affordable Care Act (ACA) saw significant reductions in uninsured rates for both racial groups, but the benefits were not equally distributed. In expansion states like Kentucky and Louisiana, Black uninsured rates dropped by over 10 percentage points, yet they still lag behind White rates due to pre-existing socioeconomic gaps. Conversely, non-expansion states like Florida and North Carolina continue to see higher uninsured rates among Black populations, with disparities widening in recent years. This suggests that policy decisions at the state level play a critical role in either mitigating or exacerbating racial inequities in coverage.
A comparative analysis of regions reveals distinct patterns. The Northeast and Midwest generally have smaller racial gaps in insurance coverage, with states like Massachusetts and Minnesota boasting near-universal coverage for both groups. These regions often have stronger safety nets, higher median incomes, and more robust public health infrastructure. In contrast, the South and parts of the West struggle with higher uninsured rates and larger disparities, driven by factors like lower wages, limited employer-sponsored insurance, and resistance to federal health policies. For example, in Alabama, 12.3% of White individuals and 16.8% of Black individuals were uninsured in 2022, reflecting both regional and racial challenges.
Practical steps to address these disparities must focus on targeted interventions. States should prioritize Medicaid expansion to cover low-income adults, particularly in the South, where many Black individuals fall into the "coverage gap" earning too much for Medicaid but too little for ACA subsidies. Employers in regions with high disparities can play a role by offering affordable health plans and educating workers about enrollment options. Community-based organizations can bridge gaps by providing culturally competent outreach and assistance with applications. Policymakers must also address systemic issues like racial bias in healthcare and economic inequality, which underpin these disparities.
In conclusion, racial disparities in health insurance coverage are not uniform but are deeply influenced by state and regional contexts. While progress has been made, persistent gaps in the South and other regions underscore the need for tailored solutions. By combining policy reforms, economic support, and community engagement, states can work toward equitable coverage, ensuring that health insurance is a right for all, regardless of race.
Consider Adding Medical to Your Auto Insurance: Here's Why
You may want to see also
Explore related products






![]()
Impact of income levels on health insurance access for Black and White populations
Income disparities between Black and White populations in the United States significantly influence health insurance access, creating a stark divide in healthcare coverage. According to the U.S. Census Bureau, as of 2022, 9.1% of non-Hispanic Whites were uninsured, compared to 9.6% of Black individuals. While these numbers appear close, they mask deeper inequities tied to income levels. For instance, among low-income households (earning below $25,000 annually), Black individuals are more likely to remain uninsured due to limited access to employer-sponsored plans and higher out-of-pocket costs for private insurance. This disparity highlights how systemic economic barriers disproportionately affect Black communities, even when overall uninsured rates seem comparable.
Consider the role of income in determining eligibility for public health insurance programs like Medicaid. While both Black and White populations benefit from Medicaid expansion under the Affordable Care Act (ACA), Black individuals are more likely to rely on these programs due to lower median household incomes. However, not all states have expanded Medicaid, leaving many low-income Black residents in a coverage gap. For example, in states like Texas and Florida, where Medicaid expansion has not been adopted, Black individuals are nearly twice as likely as Whites to remain uninsured. This geographic and income-based inequity underscores the need for targeted policy interventions to address coverage gaps in underserved communities.
A persuasive argument can be made for addressing income-based disparities through wage equity and affordable insurance options. Black workers often face wage discrimination, earning approximately 84 cents for every dollar earned by White workers, according to the Economic Policy Institute. This wage gap limits their ability to afford private health insurance, even when employer-sponsored plans are unavailable. Policymakers could mitigate this by raising the federal minimum wage to $15 per hour, as proposed in recent legislation, and expanding premium subsidies for low-income families under the ACA. Such measures would not only reduce uninsured rates but also improve health outcomes by ensuring consistent access to care.
Comparatively, middle- and high-income White households benefit from greater financial stability, enabling them to secure private health insurance more easily. For instance, 78% of Whites with incomes above $75,000 have employer-sponsored insurance, compared to 65% of Black individuals in the same income bracket. This gap persists despite similar income levels, suggesting that wealth accumulation and intergenerational financial advantages play a role. To address this, initiatives like health savings accounts (HSAs) with tax incentives could be tailored to benefit lower-income Black families, providing a financial cushion for healthcare expenses and reducing reliance on high-deductible plans.
In conclusion, income levels serve as a critical determinant of health insurance access for Black and White populations, with systemic inequities exacerbating disparities. Practical steps, such as expanding Medicaid, addressing wage gaps, and creating targeted financial tools, can help bridge this divide. By focusing on income-based solutions, policymakers and advocates can ensure that health insurance becomes a universal right rather than a privilege tied to economic status. This approach not only aligns with principles of equity but also fosters healthier, more resilient communities for all.
How HMO Transformed the Health Insurance Landscape: Key Changes Explained
You may want to see also
Explore related products






![]()
Role of employer-based insurance in coverage gaps between racial groups
Employer-based health insurance, the cornerstone of coverage for most Americans, disproportionately benefits White workers, exacerbating racial disparities in access to care. Census Bureau data from 2022 reveals that 55.4% of White individuals obtain insurance through their employer, compared to only 46.8% of Black individuals. This 8.6 percentage point gap translates to millions of Black Americans left without this critical pathway to coverage.
The root causes are multifaceted. Occupational segregation persists, with Black workers overrepresented in low-wage jobs less likely to offer health benefits. Industries like retail, hospitality, and food service, where Black workers are concentrated, often provide limited or no insurance options. Even within similar occupations, studies show Black workers are less likely to be offered employer-sponsored insurance than their White counterparts. This disparity isn't solely about job type; it's about systemic inequities embedded in hiring practices, wage structures, and benefit packages.
Consider a hypothetical scenario: two individuals, one Black and one White, both work as customer service representatives. The White employee receives health insurance through their employer, while the Black employee, despite similar qualifications and experience, works for a company that doesn't offer this benefit. This disparity, replicated across countless workplaces, contributes to the coverage gap. The Black employee may rely on more expensive individual plans, Medicaid, or go uninsured, facing financial barriers to accessing necessary care.
The consequences are dire. Without consistent coverage, Black individuals are more likely to delay preventive care, skip necessary treatments, and experience poorer health outcomes. Chronic conditions like diabetes and hypertension, prevalent in the Black community, require ongoing management, making insurance coverage crucial for disease control and quality of life.
Addressing this disparity requires a multi-pronged approach. Policymakers must incentivize employers, especially in low-wage sectors, to offer affordable health insurance options. Expanding Medicaid eligibility and strengthening public health insurance programs can provide a safety net for those excluded from employer-based coverage. Additionally, addressing occupational segregation and promoting equitable hiring practices are essential to ensuring Black workers have access to jobs with comprehensive benefits. Closing the employer-based insurance gap is not just about numbers; it's about ensuring equitable access to healthcare and ultimately, improving health outcomes for all.
Does Health Insurance Cover Motor Vehicle Accident Injuries?
You may want to see also
Explore related products


$28.95




![]()
Medicaid and Medicare enrollment differences among Black and White individuals
Racial disparities in healthcare access persist, and one critical area where this manifests is in Medicaid and Medicare enrollment. Data reveals a striking difference: Black individuals are disproportionately enrolled in Medicaid compared to their White counterparts, while White individuals dominate Medicare enrollment. This disparity isn't merely a statistical anomaly; it reflects deeper systemic inequalities in income, employment, and access to employer-sponsored insurance.
Medicaid, a needs-based program, serves as a safety net for low-income individuals and families. Historically, systemic racism has led to higher poverty rates among Black communities, making them more reliant on Medicaid for healthcare coverage. Conversely, Medicare, primarily serving individuals over 65, sees higher enrollment among Whites due to longer life expectancies and greater access to retirement benefits.
This enrollment gap has tangible consequences. Medicaid, while essential, often offers narrower provider networks and lower reimbursement rates compared to Medicare. This can translate to limited access to specialists, longer wait times, and potentially inferior health outcomes for Black individuals. Furthermore, the stigma associated with Medicaid can deter individuals from seeking necessary care, exacerbating existing health disparities.
Addressing these disparities requires a multi-pronged approach. Expanding Medicaid eligibility and improving its benefits package would significantly benefit Black communities. Simultaneously, tackling the root causes of racial inequities in income and employment is crucial for long-term solutions.
Ultimately, closing the Medicaid and Medicare enrollment gap is not just about numbers; it's about ensuring equitable access to quality healthcare for all, regardless of race. This necessitates a commitment to policy changes that address systemic racism and prioritize the health and well-being of marginalized communities.
Why Loss Runs Requests Frustrate Insurance Companies: Unveiling the Truth
You may want to see also
Explore related products






![]()
Effects of healthcare policies on insurance disparities between Black and White communities
Healthcare policies have historically shaped the insurance landscape, often exacerbating disparities between Black and White communities. For instance, the Affordable Care Act (ACA) aimed to reduce uninsured rates, but its impact was uneven. While the uninsured rate among non-Hispanic Whites dropped from 14.1% in 2013 to 7.5% in 2019, the rate for non-Hispanic Blacks decreased from 20.8% to 11.5% over the same period. This persistent gap highlights how policy implementation and structural barriers, such as access to Medicaid expansion in certain states, disproportionately affect Black communities.
Consider the role of Medicaid expansion under the ACA. States that expanded Medicaid saw larger reductions in uninsured rates, but many Southern states with significant Black populations opted out. This decision left millions of low-income Black individuals in a coverage gap, ineligible for Medicaid but unable to afford private insurance. For example, in Georgia, where 31% of the population is Black, the uninsured rate remains higher than the national average due to the state’s refusal to expand Medicaid. Policymakers must address these geographic inequities to ensure policies benefit all communities equally.
Another critical factor is the racial bias embedded in healthcare algorithms and policies. For instance, some cost-cutting algorithms used by insurers have been shown to prioritize care for White patients over Black patients with similar health needs. This systemic discrimination perpetuates disparities in insurance coverage and healthcare access. To combat this, policymakers should mandate transparency in algorithmic decision-making and enforce anti-discrimination measures in healthcare policy design.
Practical steps can be taken to mitigate these disparities. First, expand Medicaid in all states to close the coverage gap for low-income individuals. Second, increase funding for community health centers in underserved areas, which disproportionately serve Black communities. Third, implement cultural competency training for healthcare providers to reduce bias in care delivery. Finally, collect and analyze disaggregated health data by race to identify and address specific disparities. These actions, if executed thoughtfully, can begin to level the playing field in healthcare access.
In conclusion, healthcare policies have the power to either widen or narrow insurance disparities between Black and White communities. By addressing systemic barriers, geographic inequities, and racial biases, policymakers can create a more equitable healthcare system. The data is clear: targeted, inclusive policies are essential to ensuring that insurance coverage reflects the needs of all Americans, regardless of race.
Medical Membership Insurance: Understanding the Cost of Coverage
You may want to see also
Frequently asked questions
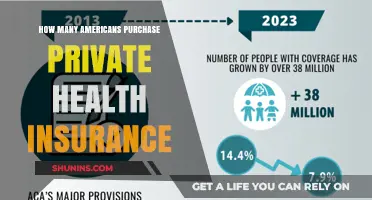
As of recent data, approximately 90-92% of Black individuals in the U.S. have health insurance, with coverage gained through employer-based plans, Medicaid, Medicare, or the Affordable Care Act (ACA) marketplace.
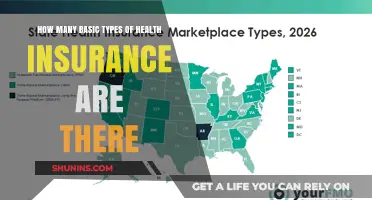
White individuals in the U.S. generally have a slightly higher health insurance rate, with about 92-94% covered, compared to 90-92% for Black individuals.
For Black individuals, the primary sources of health insurance are Medicaid (due to higher eligibility rates), employer-sponsored plans, Medicare, and ACA marketplace plans.
Yes, disparities often widen in rural areas, where Black individuals face greater challenges accessing health insurance due to limited employer-based options and fewer healthcare resources compared to White individuals.
The ACA has significantly reduced uninsured rates for both groups, but Black individuals have seen a larger percentage point decrease in uninsured rates, narrowing the gap between Black and White populations.