The issue of uninsured families remains a pressing concern in many societies, with millions of households lacking adequate health, life, or property insurance coverage. This vulnerability not only exposes families to financial ruin in the event of unforeseen circumstances, such as medical emergencies or natural disasters, but also perpetuates cycles of poverty and inequality. According to recent studies, a significant portion of the population, particularly low-income families, minorities, and those residing in rural areas, are more likely to be uninsured due to factors such as high premiums, limited access to affordable options, and lack of awareness about available programs. Understanding the scope and underlying causes of this problem is crucial in developing effective solutions to ensure that all families have access to the protection and security that insurance provides.
Explore related products






What You'll Learn
![]()
Uninsured families by income level
The gap in health insurance coverage widens significantly as income decreases, creating a stark divide in access to healthcare. Data from the U.S. Census Bureau reveals that in 2022, 14.1% of individuals in families with incomes below 138% of the federal poverty level (FPL) were uninsured, compared to only 6.5% of those in families with incomes at 400% FPL or higher. This disparity highlights how lower-income families, despite often having greater health needs, face the highest barriers to obtaining insurance.
Analyzing the reasons behind this gap, affordability emerges as the primary culprit. Even with subsidies available through the Affordable Care Act (ACA), premiums, deductibles, and copays remain out of reach for many low-income families. For instance, a family of four earning $30,000 annually (approximately 150% FPL) might still face monthly premiums exceeding $200, a significant portion of their discretionary income. Additionally, the Medicaid coverage gap in states that have not expanded Medicaid leaves millions of low-income adults ineligible for both Medicaid and ACA subsidies, further exacerbating the issue.
A comparative look at middle-income families (200–400% FPL) shows a more nuanced picture. While their uninsured rate is lower at 8.2%, they often face a different challenge: underinsurance. Many opt for high-deductible plans due to lower premiums, only to find themselves unable to afford care when needed. For example, a family with a $5,000 deductible may delay or forgo necessary treatments, leading to worse health outcomes over time. This underscores the need for policies that address not just coverage but also the affordability of care within insurance plans.
To address these disparities, practical steps can be taken. Expanding Medicaid in all states would immediately reduce the uninsured rate among low-income families by providing a safety net for those currently in the coverage gap. For middle-income families, increasing premium subsidies and capping out-of-pocket costs could make insurance more accessible and functional. Employers can also play a role by offering more affordable health plans or contributing a larger share of premiums, particularly for lower-wage workers.
In conclusion, the link between income level and insurance status is undeniable, with low-income families bearing the brunt of the uninsured crisis. By targeting affordability and expanding access to comprehensive coverage, policymakers and stakeholders can bridge this gap, ensuring that all families, regardless of income, have the healthcare they need.
Submit Evidence of Insurability to Hartford: A Step-by-Step Guide
You may want to see also
Explore related products






![]()
Geographic disparities in health insurance coverage
Across the United States, health insurance coverage varies dramatically by region, with Southern and Western states consistently reporting higher rates of uninsured families compared to the Northeast and Midwest. For instance, Texas and Florida, two of the most populous states, have uninsured rates of 18% and 13% respectively, far exceeding the national average of 9%. This disparity is not merely a statistical anomaly but a reflection of deeper systemic issues tied to state policies, economic conditions, and demographic factors. States that have expanded Medicaid under the Affordable Care Act (ACA) tend to have lower uninsured rates, while those that have not, particularly in the South, leave millions of low-income families without coverage.
Consider the rural-urban divide, a critical factor exacerbating geographic disparities. Rural areas, often concentrated in the South and Midwest, face unique challenges such as limited access to healthcare providers, lower average incomes, and fewer employer-sponsored insurance options. In contrast, urban centers, especially in the Northeast, benefit from denser healthcare networks and higher median incomes, which correlate with greater insurance coverage. For example, in Mississippi, a state with a predominantly rural population, nearly 13% of residents lack insurance, compared to just 5% in Massachusetts, a state with robust urban healthcare infrastructure and a state-run insurance marketplace.
To address these disparities, policymakers and advocates must focus on targeted interventions tailored to regional needs. Expanding Medicaid in non-expansion states could immediately reduce uninsured rates among low-income families, particularly in the South. Additionally, investing in telehealth infrastructure in rural areas could bridge the gap in access to care, though this requires reliable broadband access, which remains a challenge in many underserved regions. Employers in states with high uninsured rates could also be incentivized to offer affordable insurance plans, potentially through tax credits or subsidies.
A comparative analysis of successful state-level initiatives provides actionable insights. California, for instance, has reduced its uninsured rate to 7% through a combination of Medicaid expansion, a robust state exchange, and targeted outreach to undocumented populations. Conversely, states like Georgia, which has not expanded Medicaid, continue to struggle with uninsured rates above 12%. These examples underscore the importance of political will and policy design in mitigating geographic disparities.
Ultimately, the persistence of geographic disparities in health insurance coverage is not an insurmountable problem but a call to action. By learning from successful models, addressing rural-urban divides, and advocating for policy changes, stakeholders can work toward a more equitable healthcare system. Families in every region deserve access to affordable coverage, and achieving this goal requires a nuanced understanding of the unique challenges each area faces.
Haven Insurance Atlanta: Your Trusted Partner for Comprehensive Coverage
You may want to see also
Explore related products






![]()
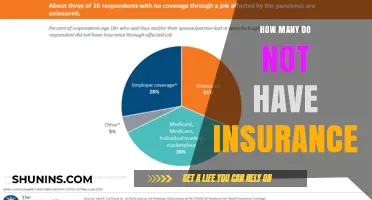
Impact of employment status on insurance
Employment status is a critical determinant of whether families have health insurance, with disparities starkly evident across different job categories. Full-time workers are significantly more likely to receive employer-sponsored insurance, the most common coverage source in the U.S. According to the U.S. Census Bureau, 67.3% of Americans had private insurance in 2022, with the majority tied to employment. Conversely, part-time workers, gig economy participants, and the self-employed often lack access to such benefits. For instance, only 25% of part-time workers receive employer-sponsored insurance, leaving many to seek costly individual plans or rely on public programs like Medicaid. This gap highlights how job structure directly influences insurance accessibility, creating a divide between the insured and uninsured.
Consider the gig economy, where workers are classified as independent contractors, stripping them of traditional employee benefits. Platforms like Uber and DoorDash offer no health insurance, forcing workers to navigate the individual market. A 2021 study by the Kaiser Family Foundation found that 40% of gig workers were uninsured or underinsured, compared to 8% of full-time employees. This vulnerability is compounded by income instability, as gig workers often cannot afford premiums or out-of-pocket costs. For families reliant on such work, the lack of insurance translates to delayed care, mounting medical debt, and heightened financial risk.
Public policy attempts to bridge this gap, but challenges persist. The Affordable Care Act (ACA) expanded Medicaid and created subsidies for individual plans, yet 2.2 million people fall into the "coverage gap" in states that did not expand Medicaid. Additionally, self-employed individuals face premiums 20-30% higher than employer-sponsored plans, despite ACA subsidies. Families in low-wage jobs often earn too much for Medicaid but too little for affordable private insurance, leaving them uninsured. This paradox underscores how employment status, combined with policy limitations, perpetuates insurance disparities.
To mitigate these issues, families can take proactive steps. First, explore ACA marketplace plans during open enrollment, using subsidies to reduce costs. For example, a family of four earning up to $106,000 annually may qualify for premium tax credits. Second, consider short-term health plans for temporary coverage, though these exclude pre-existing conditions. Third, leverage health-sharing ministries or local clinics for reduced-cost care. Employers can also play a role by offering voluntary benefits or contributing to health reimbursement arrangements (HRAs) for part-time workers. While not a panacea, these strategies provide stopgap solutions for families navigating the employment-insurance nexus.
Ultimately, the link between employment status and insurance coverage reveals systemic inequities. Full-time workers enjoy relative security, while part-time, gig, and self-employed individuals face barriers to affordable care. Policymakers must address these gaps through expanded Medicaid, portable benefits for gig workers, and enhanced subsidies for the self-employed. Until then, families must navigate a fragmented system, balancing precarious employment with the need for health security. Understanding this dynamic is the first step toward advocating for change and securing coverage in an uncertain landscape.
Prudential Life Insurance: Iconic Landmarks and Their Stories
You may want to see also
Explore related products






![]()
Racial and ethnic gaps in coverage
Racial and ethnic disparities in health insurance coverage persist as a stark reminder of systemic inequalities. According to the U.S. Census Bureau, in 2022, 8.8% of the population lacked health insurance, but this figure masks significant gaps: 9.3% of Hispanic individuals, 9.1% of American Indian and Alaska Native individuals, and 6.1% of Black individuals were uninsured, compared to 5.4% of non-Hispanic White individuals. These disparities are not coincidental but reflect deeper structural barriers to access.
To address these gaps, it’s essential to understand their root causes. Hispanic and immigrant families often face language barriers, limited employer-sponsored insurance options, and fear of enrolling in public programs due to immigration status concerns. For example, mixed-status families—where some members are citizens and others are not—may avoid programs like Medicaid or CHIP out of fear of jeopardizing their immigration status, even if eligible children qualify. Similarly, Indigenous communities face geographic isolation, with limited access to healthcare facilities and insurance navigators, exacerbating coverage gaps.
A comparative analysis reveals that policy solutions must be tailored to specific communities. Expanding Medicaid under the Affordable Care Act (ACA) significantly reduced uninsured rates, but 10 states have yet to adopt expansion, disproportionately affecting low-income communities of color. For instance, in Texas, where Medicaid expansion has not been implemented, 18% of Hispanic residents remain uninsured. In contrast, states like California, which invested in culturally competent outreach, saw sharper declines in uninsured rates among diverse populations. Practical steps include increasing funding for community health workers who speak multiple languages and understand cultural nuances, and simplifying enrollment processes for public programs.
Persuasively, closing these gaps is not just a moral imperative but an economic one. Uninsured individuals delay care, leading to costlier treatments and poorer health outcomes, which strain the healthcare system. For example, uninsured Black and Hispanic adults are less likely to receive preventive screenings, contributing to higher rates of chronic conditions like diabetes and hypertension. By ensuring equitable coverage, we reduce long-term healthcare costs and improve societal well-being. Policymakers must prioritize data-driven interventions, such as targeted subsidies for low-income families and protections against discriminatory practices in insurance markets.
Finally, a descriptive lens highlights the human impact of these disparities. Imagine a single mother in a rural Native American community, unable to afford insurance and forced to choose between medical care and feeding her children. Or a Hispanic father in a mixed-status family, forgoing coverage for his eligible children due to fear of deportation. These stories underscore the urgency of action. Practical tips for advocates include partnering with grassroots organizations to build trust, leveraging technology for outreach (e.g., multilingual apps for enrollment), and pushing for federal policies that decouple immigration status from healthcare access. Addressing racial and ethnic gaps in coverage requires both systemic change and grassroots empathy.
Does USAA Offer Condo Insurance? Coverage Options Explained
You may want to see also
Explore related products






![]()
Effects of policy changes on uninsured rates
Policy changes have a direct and measurable impact on uninsured rates, often serving as a lever to either expand or contract access to healthcare. For instance, the Affordable Care Act (ACA) of 2010 led to a significant reduction in the uninsured rate, dropping from 16% in 2010 to 8.6% in 2016, primarily through Medicaid expansion and the establishment of health insurance marketplaces. This example underscores how legislative action can reshape the healthcare landscape, particularly for low-income families who previously lacked affordable coverage options. However, the effectiveness of such policies depends on state-level adoption, as seen in the 12 states that have not expanded Medicaid, leaving millions of individuals in the "coverage gap" without affordable insurance options.
Analyzing the inverse effect, policy reversals or restrictions can swiftly erode gains in coverage. For example, the elimination of the ACA’s individual mandate penalty in 2019 contributed to a rise in uninsured rates, as fewer healthy individuals opted for coverage, destabilizing insurance markets. Similarly, changes to immigration policies, such as stricter eligibility criteria for public programs, have disproportionately affected uninsured rates among immigrant families, even those with legal status. These examples highlight the fragility of coverage gains and the need for policies that account for long-term sustainability and inclusivity.
To mitigate the negative effects of policy changes, stakeholders must adopt a multi-pronged approach. First, policymakers should prioritize data-driven decisions, such as conducting impact assessments to predict how changes will affect vulnerable populations. Second, states that have not expanded Medicaid should reconsider their stance, as doing so would immediately reduce uninsured rates by providing coverage to an estimated 2.2 million low-income adults. Third, public awareness campaigns can play a critical role in educating families about available resources, such as subsidies on health insurance marketplaces, which remain underutilized due to lack of awareness.
Comparatively, international models offer valuable lessons. Countries with universal healthcare systems, like Canada and the UK, maintain uninsured rates near zero, demonstrating the efficacy of comprehensive policy frameworks. While replicating these systems may not be feasible in the U.S., incremental steps, such as capping out-of-pocket costs or expanding eligibility for federal programs, could bridge existing gaps. For instance, lowering the Medicaid income threshold for families with children could provide immediate relief to millions, particularly in states with high uninsured rates.
Ultimately, the effects of policy changes on uninsured rates are not static but dynamic, influenced by political, economic, and social factors. Policymakers must balance fiscal responsibility with the moral imperative of ensuring access to healthcare. Families, especially those with children, are particularly vulnerable to policy shifts, as disruptions in coverage can lead to delayed care, worsened health outcomes, and financial instability. By focusing on evidence-based, inclusive policies, it is possible to create a healthcare system that protects all families, regardless of income or geography.
Life Insurance and Missing Persons: What's Covered?
You may want to see also
Frequently asked questions
As of recent data, approximately 8.5% of the U.S. population, or about 28 million people, are uninsured, which includes families without health insurance coverage.
Families often remain uninsured due to high insurance costs, lack of employer-sponsored coverage, ineligibility for public programs like Medicaid, or gaps in coverage options.
The number of uninsured families varies significantly by state, with states that have not expanded Medicaid under the Affordable Care Act (ACA) generally having higher uninsured rates.
Trends show fluctuations in uninsured rates, with decreases following ACA implementation but recent increases due to factors like rising premiums, policy changes, and economic challenges.