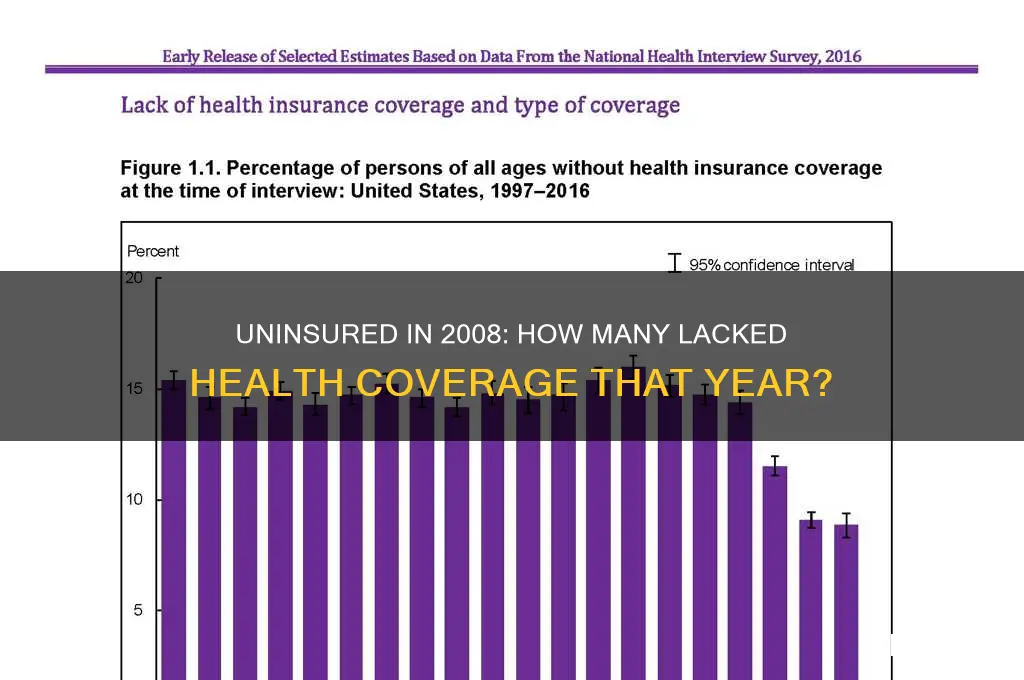
In 2008, the issue of health insurance coverage in the United States was a significant concern, with a substantial portion of the population lacking access to essential healthcare services. According to data from the U.S. Census Bureau, approximately 46.3 million people, or roughly 15.4% of the population, did not have health insurance at any point during the year. This figure highlighted the growing disparities in healthcare access, particularly among low-income individuals, part-time workers, and those employed in industries without employer-sponsored insurance. The lack of coverage not only impacted individuals' ability to receive timely medical care but also placed a considerable financial burden on the healthcare system as a whole, underscoring the urgent need for policy reforms to address this critical issue.
Explore related products






What You'll Learn
- Uninsured by Age Group: Breakdown of uninsured individuals in 2008 by age categories (e.g., children, adults)
- Uninsured by Income Level: Analysis of uninsured rates based on household income brackets in 2008
- Uninsured by State: Comparison of uninsured populations across different U.S. states in 2008
- Uninsured by Employment Status: Rates of uninsured among employed, unemployed, and part-time workers in 2008
- Uninsured by Race/Ethnicity: Disparities in uninsured rates among racial and ethnic groups in 2008
![]()
Uninsured by Age Group: Breakdown of uninsured individuals in 2008 by age categories (e.g., children, adults)
In 2008, the distribution of uninsured individuals across age groups revealed stark disparities, with young adults aged 18 to 24 bearing the brunt of the crisis. This demographic accounted for approximately 29% of the uninsured population, despite representing only 10% of the total U.S. population. The primary drivers? Transitioning off parental insurance, limited access to employer-sponsored plans, and lower enrollment in public programs like Medicaid. For instance, many college graduates entering the workforce faced gaps in coverage before securing full-time employment with benefits. This age group’s vulnerability highlights the systemic gaps in the healthcare safety net, particularly during life transitions.
Children under 18, conversely, experienced a lower uninsured rate at 8.9% in 2008, thanks largely to programs like the Children’s Health Insurance Program (CHIP). However, this still translated to over 7 million uninsured children, with disparities concentrated in low-income families and states with stricter Medicaid eligibility criteria. For example, in Texas, nearly 15% of children lacked coverage, compared to 3% in Massachusetts, which had expanded healthcare access. While progress had been made, these numbers underscore the uneven impact of policy decisions on the youngest and most vulnerable populations.
Adults aged 25 to 64 constituted the largest share of the uninsured, at 62% of the total uninsured population. Within this group, those aged 25 to 34 were particularly at risk, with 28% lacking coverage. Factors such as precarious employment, high premiums, and ineligibility for subsidies played significant roles. For instance, self-employed individuals or those in gig economy jobs often faced prohibitive costs for private insurance. Meanwhile, older adults in this category (55–64) faced a double bind: too young for Medicare but often priced out of the individual market due to pre-existing conditions.
The elderly population (65 and older) had the lowest uninsured rate, at less than 1%, due to near-universal coverage through Medicare. However, this group still faced gaps in areas like dental, vision, and long-term care, which are not fully covered by traditional Medicare. While not technically "uninsured," these omissions left many seniors financially vulnerable to out-of-pocket expenses. This contrast between near-universal coverage for seniors and the struggles of younger age groups raises questions about the equity and sustainability of the U.S. healthcare system.
Understanding the age-based breakdown of the uninsured in 2008 offers actionable insights for policymakers and advocates. Targeted interventions, such as expanding Medicaid eligibility for young adults or subsidizing premiums for low-income workers, could address specific pain points. For families with children, streamlining enrollment processes for CHIP and Medicaid could close coverage gaps. Ultimately, the data reveals not just who was left behind, but also where systemic reforms could have the greatest impact—a roadmap for building a more inclusive healthcare system.
Get Covered: Aetna Medical Insurance Application Process
You may want to see also
Explore related products






![]()
Uninsured by Income Level: Analysis of uninsured rates based on household income brackets in 2008
In 2008, approximately 46.3 million Americans lacked health insurance, a figure that underscores the pervasive challenges in accessing healthcare. However, this number alone fails to capture the disparities embedded within different income brackets. An analysis of uninsured rates by household income reveals a stark divide, with lower-income families bearing the brunt of this crisis. For instance, households earning below the federal poverty level (FPL) faced an uninsured rate of nearly 25%, compared to just 8% for those earning 400% above the FPL or more. This disparity highlights how economic status directly correlates with healthcare access.
Consider the practical implications for families in the lowest income bracket. A household of four earning below $22,050 annually in 2008 often had to choose between paying for health insurance and covering basic necessities like rent or groceries. Even subsidized programs like Medicaid, while crucial, did not fully bridge the gap due to eligibility restrictions and varying state policies. For example, in states with stricter Medicaid requirements, many low-income individuals fell into the "coverage gap," earning too much to qualify for Medicaid but too little to afford private insurance. This left them disproportionately uninsured, exacerbating health inequities.
Contrast this with households earning between 200% and 400% of the FPL, where the uninsured rate hovered around 13%. While still significant, this group often had more options, such as employer-sponsored insurance or affordable private plans. However, even here, the lack of universal coverage meant that job loss or pre-existing conditions could quickly push individuals into the uninsured category. For instance, a family earning $66,000 annually might have struggled to afford premiums for a plan covering all members, leading to partial coverage or none at all. This underscores the fragility of healthcare access even for middle-income households.
To address these disparities, policymakers and advocates must focus on targeted solutions. Expanding Medicaid eligibility, introducing income-based subsidies, and creating more affordable insurance options could significantly reduce uninsured rates among low-income populations. For middle-income households, stabilizing the individual insurance market and capping premium costs could provide much-needed relief. By understanding the income-based nuances of uninsured rates in 2008, we can design interventions that address the root causes of this issue, ensuring that healthcare becomes a right, not a privilege, for all income levels.
Meet the CEO of United American Insurance Company: Leadership Insights
You may want to see also
Explore related products






![]()
Uninsured by State: Comparison of uninsured populations across different U.S. states in 2008
In 2008, approximately 46.3 million Americans lacked health insurance, a figure that varied significantly across states, reflecting disparities in economic conditions, policy environments, and demographic compositions. Texas led the nation with the highest number of uninsured individuals, surpassing 6 million, largely due to its large population and limited Medicaid expansion. In contrast, Massachusetts, with its groundbreaking health reform implemented in 2006, boasted the lowest uninsured rate at 4.1%, demonstrating the impact of state-level policy interventions. These extremes highlight the critical role of regional factors in shaping access to healthcare.
Analyzing the data reveals a clear divide between states with robust safety nets and those with more restrictive policies. Southern and Western states, such as New Mexico, Florida, and Nevada, consistently ranked among the highest in uninsured rates, often exceeding 20%. These states often had lower Medicaid eligibility thresholds and fewer resources allocated to public health programs. Conversely, Northeastern states like Vermont and Maine, with more expansive Medicaid coverage and proactive outreach efforts, maintained uninsured rates below 10%. This comparison underscores the influence of state-level decisions on health equity.
A closer look at demographic trends within states provides additional insights. In Texas, for instance, nearly 25% of the Hispanic population was uninsured, compared to 15% of the white population, reflecting broader national disparities in access. Similarly, in California, young adults aged 18–24 were disproportionately uninsured, with rates nearing 30%, likely due to gaps in employer-sponsored coverage and limited eligibility for public programs. These patterns suggest that state-level data must be disaggregated to address specific vulnerabilities within populations.
For policymakers and advocates, understanding these state-by-state variations is essential for crafting targeted solutions. States with high uninsured rates could emulate Massachusetts’ model by expanding Medicaid, implementing health insurance mandates, or investing in community health programs. Additionally, addressing demographic disparities requires culturally competent outreach and tailored policies, such as language-specific enrollment assistance or income-based subsidies. By learning from both the successes and challenges of 2008, states can work toward reducing uninsured rates and improving health outcomes for all residents.
Finally, the 2008 data serves as a baseline for evaluating progress in the years following the Affordable Care Act’s implementation in 2010. While national uninsured rates have since declined, the state-level disparities observed in 2008 persist, reminding us that one-size-fits-all approaches are insufficient. Practical steps for states include conducting regular needs assessments, collaborating with local organizations, and leveraging federal funding opportunities. By prioritizing equity and adaptability, states can build on the lessons of 2008 to ensure that health insurance becomes a universal reality, not a geographic privilege.
No Marketplace Health Insurance? Understanding Form 1095-S Requirements
You may want to see also
Explore related products






![]()
Uninsured by Employment Status: Rates of uninsured among employed, unemployed, and part-time workers in 2008
In 2008, the employment status of individuals played a significant role in determining their likelihood of being uninsured. Data from the U.S. Census Bureau reveals a stark disparity: while 10.3% of full-time workers lacked health insurance, a staggering 28.6% of part-time workers and 30.6% of unemployed individuals were uninsured. This gap underscores the precarious nature of health coverage for those outside traditional full-time employment.
Consider the part-time workforce, often comprising students, caregivers, or those unable to secure full-time positions. Many part-time jobs do not offer employer-sponsored health insurance, leaving workers to navigate the costly individual market or rely on public programs with strict eligibility criteria. For instance, a 25-year-old part-time retail worker earning $15,000 annually might not qualify for Medicaid in states with restrictive income limits and cannot afford a private plan averaging $3,500 annually. This example illustrates how employment status directly correlates with access to affordable coverage.
Unemployed individuals face even greater challenges. Without employer-sponsored insurance, they must turn to COBRA, which allows them to continue their previous employer’s plan but at full cost, often exceeding $500 monthly for individual coverage. Alternatively, they may seek Medicaid or state-based programs, but eligibility varies widely. For example, in 2008, a 40-year-old unemployed worker in Texas with no children and an income above the poverty line would likely fall into the "coverage gap," ineligible for both Medicaid and subsidies on the individual market.
Employed individuals are not immune to these disparities. While full-time workers are more likely to have employer-sponsored insurance, small businesses employing fewer than 50 workers are not mandated to provide coverage. This leaves employees in such firms at higher risk of being uninsured. For instance, a full-time worker at a small landscaping company might earn too much to qualify for Medicaid but not enough to afford a private plan, highlighting the limitations of employment-based coverage.
To address these gaps, policymakers and employers must consider targeted solutions. Expanding Medicaid eligibility, subsidizing individual market plans for low-income workers, and incentivizing small businesses to offer health benefits could reduce disparities. For individuals, understanding eligibility for public programs and exploring health insurance cooperatives or short-term plans (with caution) can provide temporary relief. Ultimately, the 2008 data serves as a reminder that employment status is a critical determinant of health insurance access, demanding tailored interventions to ensure coverage for all.
Does Health Insurance Cover Liposuction? Understanding Coverage and Costs
You may want to see also
Explore related products




![Life and Health Insurance Study Cards: Life Health Insurance License Exam Prep with Practice Test Questions [Full Color]](https://m.media-amazon.com/images/I/51Pox87Z5lL._AC_UL320_.jpg)

![]()
Uninsured by Race/Ethnicity: Disparities in uninsured rates among racial and ethnic groups in 2008
In 2008, racial and ethnic disparities in health insurance coverage revealed stark inequalities, with Hispanic individuals experiencing the highest uninsured rates at 30.7%, nearly triple the rate of non-Hispanic whites (11.5%). This gap underscores systemic barriers to access, including employment in low-wage jobs without benefits and immigration status restrictions. For instance, many Hispanic workers were employed in sectors like agriculture and hospitality, where employer-sponsored insurance is rare, leaving them disproportionately vulnerable.
Analyzing the data further, non-Hispanic Blacks also faced significant disparities, with an uninsured rate of 19.1%, nearly double that of non-Hispanic whites. This reflects historical and ongoing socioeconomic inequities, such as lower median incomes and reduced access to stable, benefit-providing employment. In contrast, Asian Americans had an uninsured rate of 17.6%, a figure that masks internal diversity—some subgroups, like Southeast Asian communities, faced higher rates due to language barriers and recent immigration status, while others, like Chinese Americans, had lower rates tied to higher educational attainment and professional occupations.
Native American and Alaska Native populations experienced an uninsured rate of 28.3%, the second-highest among all groups. This is compounded by the underfunding of the Indian Health Service, which, despite treaty obligations, often lacks resources to meet the full healthcare needs of these communities. For example, many Native Americans live in rural areas with limited access to healthcare facilities, further exacerbating their vulnerability.
Addressing these disparities requires targeted policy interventions. Expanding Medicaid eligibility, as later implemented under the Affordable Care Act, could have significantly reduced uninsured rates among low-income Hispanic and Black populations. Additionally, culturally competent outreach programs and language services could improve enrollment among non-English-speaking communities. For Native Americans, honoring federal trust responsibilities by fully funding the Indian Health Service is essential.
In conclusion, the 2008 uninsured rates by race and ethnicity highlight systemic inequities rooted in employment, immigration policy, and historical injustices. Practical steps, such as policy reforms and targeted outreach, can begin to bridge these gaps, ensuring that health insurance coverage is a right for all, regardless of race or ethnicity.
Understanding Per Diem Insurance and Medical Expense Deductions
You may want to see also
Frequently asked questions
In 2008, approximately 46.3 million people in the United States were uninsured, according to data from the U.S. Census Bureau.
About 15.4% of the U.S. population, or roughly one in six Americans, lacked health insurance in 2008.
The number of uninsured people increased in 2008 compared to 2007, rising by about 600,000 individuals, according to Census Bureau data.
Young adults (aged 18–24), low-income individuals, and Hispanic or Latino populations were among the groups most likely to be uninsured in 2008.
The 2008 recession contributed to the rise in uninsured individuals, as job losses led to the loss of employer-sponsored health insurance for many Americans.