The question of how many people in the world have health insurance is a critical yet complex issue, reflecting disparities in global healthcare access and socioeconomic conditions. As of recent estimates, approximately 5.8 billion people, or about 75% of the world’s population, have some form of health insurance or coverage, primarily through government-funded systems, employer-based plans, or private policies. However, this figure masks significant inequalities, as coverage is heavily concentrated in high-income countries, while low- and middle-income nations often struggle with limited access, leaving billions vulnerable to financial hardship due to out-of-pocket medical expenses. Understanding these disparities is essential for addressing global health inequities and working toward universal health coverage.
Explore related products






What You'll Learn
![]()
Global health insurance coverage statistics
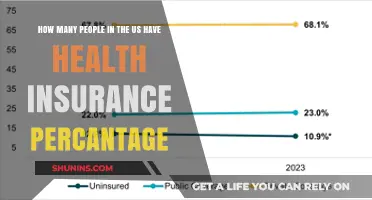
Global health insurance coverage is a patchwork of disparities, with approximately 4.5 billion people—or roughly 58% of the world’s population—having some form of health insurance or access to healthcare services. This statistic, drawn from World Health Organization (WHO) and World Bank data, highlights a stark divide: high-income countries like Germany, Japan, and Canada boast near-universal coverage, while low-income nations in sub-Saharan Africa and parts of Asia see coverage rates below 20%. The primary drivers of this gap include economic inequality, government investment in healthcare infrastructure, and the prevalence of employer-based insurance models. For instance, in the United States, 91% of the population is insured, yet out-of-pocket costs remain a barrier for many, illustrating that coverage does not always equate to affordability or accessibility.
To understand these disparities, consider the role of government-led initiatives. Countries with single-payer systems, such as the UK’s National Health Service (NHS), achieve near-universal coverage by pooling public funds to provide free-at-point-of-service care. In contrast, India’s Ayushman Bharat scheme, launched in 2018, aims to cover 500 million low-income citizens but faces challenges in implementation and awareness. Meanwhile, in Africa, Rwanda’s community-based health insurance program, *Mutuelle de Santé*, has increased coverage to 80% of its population, demonstrating the impact of localized, low-cost solutions. These examples underscore the importance of tailored policies that address regional economic and cultural contexts.
A critical takeaway is that health insurance coverage is not merely a numbers game but a measure of equity and resilience. In high-income countries, the focus is shifting from *coverage* to *quality of care*, with metrics like wait times and patient outcomes taking precedence. Conversely, low-income nations prioritize *access*, often relying on international aid and NGOs to bridge gaps. For instance, the Global Fund has provided health insurance subsidies to 20 million people in low-resource settings, primarily for HIV/AIDS, tuberculosis, and malaria treatment. This dual focus—expanding access in underserved regions while improving care standards globally—is essential for achieving the UN’s Sustainable Development Goal 3: Good Health and Well-being.
Practical steps to improve global coverage include leveraging technology, such as mobile health platforms, to reach remote populations. Kenya’s *M-TIBA* system, for example, allows users to save, send, and spend funds specifically for healthcare via mobile phones, benefiting 4 million users since 2015. Additionally, policymakers should incentivize private insurers to offer affordable plans in underserved markets, as seen in Ghana’s partnership with private insurers to expand the National Health Insurance Scheme. Caution, however, must be taken to avoid over-reliance on private models, which can exacerbate inequalities if not regulated. Ultimately, a balanced approach—combining public funding, private innovation, and community engagement—is key to closing the global health insurance gap.
Verify Your Medical Insurance Status: Quick and Easy Steps
You may want to see also
Explore related products






![]()
Regional disparities in health insurance access
Health insurance coverage varies dramatically across regions, with high-income countries like Germany, Japan, and Canada achieving near-universal access, while low-income nations in sub-Saharan Africa and parts of Asia struggle with coverage rates below 10%. This disparity is not merely a statistical gap but a reflection of deeper systemic inequalities in healthcare infrastructure, economic resources, and policy priorities. For instance, in Germany, mandatory health insurance laws ensure that 99% of the population is covered, whereas in Nigeria, only 5% of citizens have formal health insurance, leaving the majority reliant on out-of-pocket payments that often lead to financial hardship.
Consider the role of government policy in shaping these disparities. In countries like the United Kingdom, the National Health Service (NHS) provides universal coverage funded by taxation, eliminating the need for private insurance. In contrast, the United States, despite being a high-income nation, has a fragmented system where 9% of the population remains uninsured due to the reliance on employer-based insurance and high premiums. This highlights how political decisions—whether to prioritize universal coverage or market-driven systems—directly influence access. For policymakers in low-income regions, studying models like Thailand’s Universal Coverage Scheme, which achieved 98% coverage through a mix of taxation and subsidies, could offer actionable insights.
Economic factors further exacerbate regional disparities. In India, where 80% of health expenditure is out-of-pocket, the poor often forgo necessary care due to cost. Meanwhile, in Scandinavian countries, robust social welfare systems ensure that health insurance is both affordable and comprehensive. A practical step for low-income nations could be implementing community-based health insurance schemes, as seen in Rwanda, where coverage increased from 9% to 79% in a decade. Such schemes pool resources locally, reducing individual financial burden while fostering collective responsibility.
Cultural and geographic barriers also play a significant role. In rural areas of Latin America and Africa, physical distance from healthcare facilities and lack of awareness about insurance options limit access. For example, in Peru, urban residents are twice as likely to have insurance as their rural counterparts. Addressing this requires not just policy changes but innovative solutions like mobile clinics and digital health platforms. A takeaway for stakeholders: invest in infrastructure and education to bridge the urban-rural divide, ensuring that insurance is not just available but accessible.
Finally, global health initiatives must prioritize reducing these disparities. Organizations like the World Health Organization (WHO) advocate for universal health coverage, but implementation requires tailored approaches. High-income nations can contribute through funding and knowledge-sharing, while low-income countries must focus on sustainable, context-specific solutions. For instance, leveraging technology to streamline insurance enrollment and claims processing could be a game-changer in regions with limited administrative capacity. The ultimate goal? A world where health insurance is a right, not a privilege, regardless of geography.
Why GoodRx Often Beats Company Insurance for Prescription Savings
You may want to see also
Explore related products






![]()
Impact of income on insurance ownership
Income is a critical determinant of health insurance ownership, shaping access to healthcare across the globe. Data from the World Bank and World Health Organization reveal a stark disparity: in high-income countries, over 90% of the population has some form of health insurance, while in low-income countries, this figure drops to less than 10%. This gap underscores how financial resources directly correlate with the ability to secure health coverage. For instance, in the United States, where employer-sponsored insurance is common, individuals in higher income brackets are more likely to have comprehensive plans, whereas lower-income households often rely on Medicaid or remain uninsured due to affordability issues.
The relationship between income and insurance ownership is not linear but influenced by systemic factors. In middle-income countries like India and Brazil, government-led initiatives have expanded coverage, yet out-of-pocket expenses remain a barrier for the poorest quintiles. For example, in India, despite the Ayushman Bharat scheme aiming to cover 500 million people, many low-income families still forgo insurance due to hidden costs like transportation to healthcare facilities. This highlights how income not only determines access to insurance but also the ability to utilize it effectively.
From a practical standpoint, increasing insurance ownership among low-income populations requires targeted interventions. Subsidized premiums, community-based health savings plans, and microinsurance models have shown promise in countries like Kenya and the Philippines. For instance, Kenya’s M-TIBA platform allows users to save and pay for healthcare via mobile money, making insurance more accessible to informal workers. Such innovations demonstrate that addressing income disparities in insurance ownership demands both policy support and technological solutions tailored to local contexts.
A comparative analysis of high- and low-income countries reveals that income inequality exacerbates insurance gaps. In countries with high Gini coefficients, such as South Africa, the wealthiest 20% are nearly five times more likely to have insurance than the poorest 20%. Conversely, nations with progressive taxation and universal healthcare systems, like Sweden, achieve near-universal coverage regardless of income. This suggests that redistributive policies can mitigate the impact of income on insurance ownership, offering a pathway to greater health equity.
Ultimately, the impact of income on insurance ownership is a reflection of broader socioeconomic inequalities. While income remains a primary barrier, it is not insurmountable. By combining policy reforms, technological innovations, and community-driven approaches, it is possible to expand coverage to underserved populations. Practical steps include implementing income-based subsidies, promoting health literacy, and fostering public-private partnerships to create affordable insurance products. Addressing this issue is not just a matter of financial inclusion but a critical step toward achieving global health equity.
Medical Insurance for Canada: What's the Cost?
You may want to see also
Explore related products






![]()
Government vs. private insurance prevalence
The global health insurance landscape is a patchwork of government-funded and private systems, each with distinct prevalence rates and implications for coverage. In high-income countries like Canada and the UK, government-funded insurance dominates, covering over 90% of the population. These systems, often tax-based, prioritize universal access but may face challenges like long wait times for non-emergency care. Conversely, in the United States, private insurance prevails, covering approximately 68% of the population, while government programs like Medicare and Medicaid serve specific demographics, leaving about 8% uninsured. This contrast highlights how policy choices shape insurance prevalence and health equity.
Analyzing the prevalence of government versus private insurance reveals a correlation with healthcare outcomes and costs. Countries with strong government-funded systems, such as Germany and Japan, achieve near-universal coverage while maintaining lower per capita healthcare spending compared to the U.S. For instance, Germany’s multi-payer statutory health insurance system covers 90% of its population, with private insurance catering to higher-income individuals. In contrast, private insurance-dominated systems often struggle with affordability, as seen in the U.S., where premiums and out-of-pocket costs are among the highest globally. This suggests that government-led models may offer more cost-effective and inclusive solutions.
For individuals navigating insurance options, understanding the prevalence of government versus private systems is crucial. In countries with robust government insurance, like Australia’s Medicare, enrolling is straightforward, often automatic, and provides comprehensive coverage for most services. However, private insurance may still be sought for additional benefits like private hospital rooms or reduced wait times. In private insurance-heavy markets, such as India, where government coverage is limited, individuals must carefully assess policies for coverage limits, exclusions, and premiums. Practical tips include comparing provider networks, checking for pre-existing condition clauses, and leveraging employer-sponsored plans where available.
A comparative analysis of government and private insurance prevalence underscores the role of cultural and political factors. In Scandinavian countries, high trust in government and a strong welfare state ethos have fostered near-universal public insurance. Conversely, in the U.S., historical reliance on employer-based private insurance and ideological resistance to government intervention have shaped its fragmented system. Emerging economies like Brazil and South Africa illustrate hybrid models, where government insurance coexists with private options, often catering to different socioeconomic groups. These examples demonstrate that prevalence is not just a policy outcome but a reflection of societal values and priorities.
To address gaps in insurance prevalence, policymakers and stakeholders must consider tailored strategies. In regions with low government insurance penetration, incremental reforms like expanding eligibility for public programs or introducing subsidies for private plans can improve coverage. For instance, Rwanda’s community-based health insurance scheme has achieved over 80% coverage by combining government funding with affordable premiums. In private insurance-dominated markets, regulating pricing practices and mandating essential benefits can enhance accessibility. Ultimately, balancing government and private insurance prevalence requires a nuanced approach that aligns with local needs, resources, and cultural contexts.
Grady Hospital Insurance: Application Process Simplified
You may want to see also
Explore related products






![]()
Uninsured population trends worldwide
The global uninsured population remains a pressing concern, with an estimated 4.5 billion people lacking adequate health insurance coverage. This figure, while staggering, masks significant regional disparities and evolving trends that demand attention. In low-income countries, particularly in sub-Saharan Africa and parts of Asia, uninsured rates often exceed 80%, driven by limited healthcare infrastructure and economic constraints. Conversely, high-income nations like Germany and Japan boast near-universal coverage, highlighting the impact of robust public health systems. However, even in wealthier regions, gaps persist, with the United States serving as a notable example where approximately 8.5% of the population remains uninsured despite its economic prowess.
Analyzing trends reveals a slow but steady decline in the uninsured population globally, primarily due to expanded public health initiatives in emerging economies. For instance, India’s Ayushman Bharat scheme aims to cover 500 million vulnerable citizens, while Indonesia’s JKN program has extended coverage to over 80% of its population. These efforts, however, are often hampered by funding shortfalls and administrative inefficiencies. In contrast, some middle-income countries, such as Brazil and South Africa, have seen stagnation or even slight increases in uninsured rates due to economic downturns and political instability. This underscores the fragility of progress in the absence of sustained commitment and resources.
A comparative analysis of uninsured populations across age groups reveals that young adults (18–34 years) are disproportionately affected, particularly in countries with fragmented healthcare systems. In the U.S., this demographic accounts for nearly 40% of the uninsured, often due to the high cost of private insurance and ineligibility for public programs. Conversely, children in many low-income nations face higher uninsured rates, with UNICEF reporting that over 50% of children in sub-Saharan Africa lack access to essential health services. Addressing these disparities requires targeted policies, such as subsidizing premiums for young adults and expanding pediatric care in underserved regions.
Persuasively, the moral and economic case for reducing the uninsured population is undeniable. Uninsured individuals are more likely to delay care, leading to worse health outcomes and higher long-term costs for healthcare systems. For example, untreated chronic conditions like diabetes or hypertension can result in complications requiring expensive interventions. Moreover, the COVID-19 pandemic exposed the vulnerabilities of fragmented systems, as uninsured populations faced barriers to testing and vaccination, prolonging the crisis. Investing in universal health coverage not only improves public health but also fosters economic stability by reducing absenteeism and increasing productivity.
Practically, reducing the uninsured population requires a multi-faceted approach. Governments must prioritize funding for public health programs while incentivizing private sector participation. For instance, tax credits for employers offering health insurance can expand coverage in the formal sector. Additionally, leveraging technology, such as mobile health clinics and telemedicine, can bridge gaps in rural and underserved areas. Individuals can also take proactive steps, such as exploring community health programs or pooling resources through cooperatives. Ultimately, the goal is not just to reduce numbers but to ensure equitable access to quality healthcare for all, regardless of geography or income.
Does German Health Insurance Cover Orthopedic Stem Cell Therapy?
You may want to see also
Frequently asked questions
As of recent estimates, approximately 5.4 billion people worldwide have some form of health insurance, though coverage varies significantly by region and country.
About 70% of the global population has health insurance, but this figure includes both public and private coverage, with disparities between high-income and low-income countries.
High-income countries, particularly in Europe and North America, have the highest rates of health insurance coverage, often exceeding 90%. In contrast, low-income regions, especially in sub-Saharan Africa and parts of Asia, have the lowest rates, with coverage sometimes below 20%.