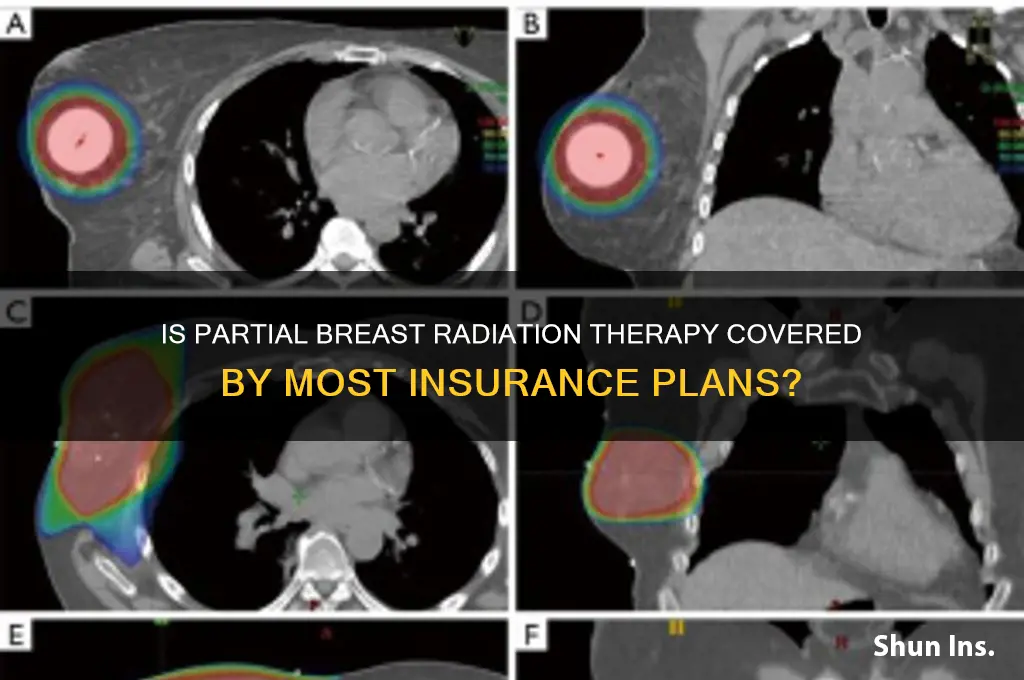
Partial breast radiation therapy (PBRT) is an innovative treatment option for early-stage breast cancer, offering a more targeted and shorter course of radiation compared to traditional whole breast radiation. Despite its proven efficacy and potential benefits, such as reduced treatment time and fewer side effects, acceptance by insurance providers remains a critical concern for many patients. While some major insurers have begun covering PBRT, coverage policies vary widely, often depending on the specific insurance plan, geographic location, and the type of PBRT technique used. Patients and healthcare providers must navigate these complexities to ensure access to this advanced treatment, highlighting the need for clearer guidelines and broader insurance acceptance to make PBRT a more accessible option for eligible individuals.
| Characteristics | Values |
|---|---|
| Insurance Coverage | Most major insurance plans, including Medicare, cover partial breast radiation therapy (PBRT). |
| FDA Approval | PBRT is FDA-approved for early-stage breast cancer treatment. |
| Clinical Guidelines | Supported by ASTRO (American Society for Radiation Oncology) guidelines. |
| Cost-Effectiveness | Generally more cost-effective than whole breast radiation therapy (WBRT). |
| Treatment Duration | Shorter treatment time (3-5 days) compared to WBRT (3-6 weeks). |
| Patient Eligibility | Typically recommended for patients with early-stage, low-risk breast cancer. |
| Outcomes | Comparable efficacy to WBRT in terms of local control and survival rates. |
| Side Effects | Fewer acute side effects compared to WBRT, but long-term data still evolving. |
| Provider Availability | Increasingly available at cancer centers and hospitals across the U.S. |
| Patient Preference | Often preferred by patients due to convenience and reduced treatment time. |
| Ongoing Research | Continued studies to expand eligibility criteria and refine techniques. |
Explore related products






What You'll Learn
- Insurance Coverage Trends: Major insurers increasingly cover partial breast radiation therapy due to proven efficacy and cost-effectiveness
- Medicare Acceptance: Medicare typically covers partial breast radiation, ensuring accessibility for eligible patients nationwide
- Private Insurer Policies: Most private insurers include partial breast radiation in their standard oncology treatment coverage plans
- Out-of-Pocket Costs: Coverage reduces patient out-of-pocket expenses, making treatment more affordable and accessible
- Clinical Evidence Impact: Strong clinical data supports insurance acceptance, driving broader coverage for partial breast radiation
![]()
Insurance Coverage Trends: Major insurers increasingly cover partial breast radiation therapy due to proven efficacy and cost-effectiveness
Partial breast radiation therapy (PBRT) has emerged as a focal point in the evolving landscape of cancer treatment coverage, with major insurers increasingly recognizing its value. This shift is driven by compelling clinical evidence demonstrating PBRT’s efficacy in treating early-stage breast cancer, often with fewer side effects compared to whole breast radiation. For instance, studies show that PBRT delivers a targeted dose of 30–34 Gy over 3–5 days, significantly reducing treatment duration compared to the 5–7 weeks required for traditional whole breast radiation. This efficiency not only improves patient compliance but also aligns with insurers’ focus on cost-effective solutions.
The financial implications of PBRT adoption are a key factor in its growing acceptance. By shortening treatment timelines, PBRT reduces associated costs, including fewer clinic visits and lower indirect expenses like lost wages for patients. Insurers such as UnitedHealthcare, Aetna, and Cigna have expanded coverage for PBRT, citing its ability to achieve comparable outcomes to conventional methods at a fraction of the cost. For example, a 2022 analysis revealed that PBRT could save up to $5,000 per patient compared to whole breast radiation, making it an attractive option for both payers and patients.
Despite its advantages, the transition to widespread coverage has not been uniform. Smaller insurers and regional plans may still require pre-authorization or impose restrictions based on patient age, tumor characteristics, or treatment history. Patients aged 50 and older with early-stage, hormone receptor-positive tumors are typically ideal candidates for PBRT, but individual policies can vary. To navigate these discrepancies, patients are advised to consult their insurance provider directly and work with their oncologist to submit detailed treatment plans that highlight PBRT’s clinical and economic benefits.
The trend toward broader PBRT coverage reflects a larger shift in healthcare toward value-based care, where treatments are evaluated not just on clinical outcomes but also on their impact on quality of life and system-wide costs. As more insurers adopt this perspective, PBRT is poised to become a standard option for eligible patients. Practical tips for patients include verifying coverage specifics, exploring appeals processes if initially denied, and leveraging advocacy groups that provide resources on negotiating insurance approvals. This proactive approach ensures that patients can access the most effective and efficient treatment available.
Does Travis Scott Have Insurance? Exploring His Coverage After Astroworld
You may want to see also
Explore related products



![]()
Medicare Acceptance: Medicare typically covers partial breast radiation, ensuring accessibility for eligible patients nationwide
Partial breast radiation therapy (PBRT) has emerged as a targeted, less invasive alternative to whole breast radiation for early-stage breast cancer patients. For many, the question of insurance coverage is pivotal in deciding treatment options. Medicare, a cornerstone of healthcare for Americans aged 65 and older, plays a critical role in this landscape. Its acceptance of PBRT ensures that eligible patients nationwide can access this advanced treatment without prohibitive out-of-pocket costs. This coverage is particularly significant given that breast cancer is most commonly diagnosed in women over 50, a demographic heavily reliant on Medicare.
Medicare’s coverage of PBRT is rooted in its recognition of the therapy’s clinical efficacy and patient benefits. Typically, Medicare Part B covers radiation therapy, including PBRT, when it is deemed medically necessary. This includes cases where the patient has undergone lumpectomy for early-stage, invasive breast cancer or ductal carcinoma in situ (DCIS). The therapy is often delivered in shorter treatment cycles—ranging from 1 to 5 days—compared to the 5-7 weeks required for traditional whole breast radiation. This condensed schedule not only reduces treatment burden but also aligns with Medicare’s focus on cost-effective, evidence-based care.
To qualify for Medicare coverage, patients must meet specific criteria. First, the cancer must be early-stage, with no evidence of spread to lymph nodes or other tissues. Second, the patient must have undergone a successful lumpectomy, and PBRT must be recommended by an oncologist as part of the treatment plan. Medicare typically covers 80% of the approved amount for the procedure, leaving the patient responsible for the remaining 20% after the deductible is met. However, supplemental insurance plans, such as Medigap, can further offset these costs, making PBRT financially feasible for most Medicare beneficiaries.
Practical considerations for patients include verifying coverage details with their Medicare provider and ensuring the treatment facility is Medicare-approved. Patients should also discuss the specific PBRT technique—whether it’s brachytherapy, external beam radiation, or intraoperative radiation—with their healthcare team, as these may have varying coverage nuances. Additionally, Medicare Advantage plans, offered by private insurers, often include PBRT coverage but may require prior authorization. Understanding these details can streamline the treatment process and minimize unexpected expenses.
In summary, Medicare’s acceptance of partial breast radiation therapy removes a significant barrier to accessing this innovative treatment. By covering PBRT for eligible patients, Medicare ensures that older adults, who constitute a substantial portion of breast cancer diagnoses, can benefit from a therapy that is both clinically effective and less disruptive to daily life. For patients navigating treatment decisions, Medicare’s coverage provides a critical safety net, making PBRT a viable and accessible option nationwide.
QuickBooks Guide: Recording Insurance Loss Entries Step-by-Step
You may want to see also
Explore related products


![]()
Private Insurer Policies: Most private insurers include partial breast radiation in their standard oncology treatment coverage plans
Partial breast radiation therapy (PBRT) has emerged as a targeted, less invasive alternative to whole breast radiation for early-stage breast cancer patients. For those weighing treatment options, insurance coverage is a critical factor. Fortunately, most private insurers now include PBRT in their standard oncology treatment coverage plans, reflecting its growing acceptance in clinical practice. This shift is supported by evidence demonstrating PBRT’s efficacy in reducing tumor recurrence while minimizing exposure to healthy tissue, aligning with insurers’ goals of cost-effective, patient-centered care.
From an analytical perspective, the inclusion of PBRT in private insurance plans is driven by both clinical and economic considerations. Studies show that PBRT, often delivered via brachytherapy or external beam techniques, achieves comparable outcomes to whole breast radiation for eligible patients, typically those with unifocal tumors ≤3 cm, clear margins, and no lymph node involvement. Insurers recognize that PBRT’s shorter treatment duration (3–5 days vs. 3–6 weeks) reduces costs associated with prolonged therapy, making it a financially viable option. For example, a 2022 analysis found that PBRT saved insurers an average of $2,500 per patient compared to traditional radiation protocols.
Patients considering PBRT should proactively verify their coverage by reviewing their policy’s oncology treatment section or contacting their insurer directly. While most private plans cover PBRT, some may impose restrictions based on age (typically 45+), tumor characteristics, or treatment facility accreditation. For instance, insurers often require PBRT to be administered in facilities accredited by the American College of Radiology (ACR) or using FDA-approved devices like the MammoSite applicator. Patients should also confirm if pre-authorization is required to avoid unexpected out-of-pocket expenses.
A persuasive argument for PBRT’s inclusion in insurance plans lies in its patient-centric benefits. Unlike whole breast radiation, PBRT significantly reduces skin irritation, fatigue, and disruption to daily life, improving adherence and quality of life. For older patients or those with comorbidities, this minimally invasive approach is particularly advantageous. Insurers that cover PBRT not only support evidence-based care but also enhance patient satisfaction, a key metric in value-based healthcare models. For example, a 2021 survey found that 89% of PBRT patients reported high treatment satisfaction compared to 72% of whole breast radiation recipients.
In conclusion, the widespread inclusion of partial breast radiation therapy in private insurer policies reflects its established role in modern breast cancer care. Patients and providers alike benefit from this coverage, which ensures access to a proven, cost-effective treatment option. By understanding their policy specifics and advocating for PBRT when appropriate, patients can make informed decisions that balance clinical outcomes with financial feasibility. As insurers continue to prioritize value-based care, PBRT’s coverage is likely to remain a standard feature of oncology treatment plans.
Canceling RBC Life Insurance: A Step-by-Step Guide
You may want to see also
Explore related products


$8.99 $19.99



![]()
Out-of-Pocket Costs: Coverage reduces patient out-of-pocket expenses, making treatment more affordable and accessible
Partial breast radiation therapy (PBRT) has emerged as a targeted, less invasive alternative to whole breast radiation, offering shorter treatment durations and potentially fewer side effects. However, its adoption hinges significantly on insurance coverage, which directly impacts patient out-of-pocket costs. Without coverage, patients may face substantial financial burdens, ranging from $5,000 to $15,000, depending on the treatment modality and geographic location. For instance, brachytherapy, a common PBRT technique, can cost up to $10,000 out-of-pocket if not covered, while external beam PBRT may range from $6,000 to $8,000. These expenses can deter eligible patients, particularly those with high-deductible plans or limited financial resources, from choosing PBRT over traditional treatments.
Insurance coverage acts as a critical buffer against these costs, reducing patient expenses to manageable copays or coinsurance rates. For example, a patient with a Platinum-level plan might pay as little as 10% of the total cost, while those with Bronze plans could still see reductions from $15,000 to $3,000–$5,000. This financial relief not only makes PBRT more accessible but also encourages adherence to treatment plans, improving outcomes for early-stage breast cancer patients, particularly those aged 50–70, who are prime candidates for this therapy. However, coverage variability across insurers and states means patients must navigate complex policies, often requiring pre-authorization or appeals to secure benefits.
To maximize affordability, patients should proactively verify their insurance benefits before starting treatment. Key steps include contacting their insurer to confirm PBRT coverage under their specific plan, understanding deductibles and out-of-pocket maximums, and inquiring about in-network providers. For instance, some insurers may cover intraoperative radiation therapy (IORT) but exclude other PBRT methods, such as 3D conformal radiation therapy. Additionally, patients can explore financial assistance programs offered by hospitals or nonprofit organizations, which may provide grants or payment plans to offset remaining costs. Practical tips include requesting a detailed cost estimate from the treatment facility and comparing it with insurance explanations of benefits to identify potential discrepancies.
The persuasive case for broader insurance coverage of PBRT lies in its long-term cost-effectiveness and patient-centered benefits. Studies show that PBRT reduces treatment time from 6–7 weeks to just 5 days, minimizing lost wages and caregiver expenses for patients and their families. For example, a 55-year-old working professional could save approximately $2,000 in unpaid leave by opting for PBRT over whole breast radiation. Insurers that embrace coverage not only enhance patient access but also align with value-based care models, prioritizing outcomes over treatment duration. Advocacy efforts, including patient testimonials and clinical data, can further pressure insurers to standardize PBRT coverage, ensuring equitable access regardless of socioeconomic status.
In conclusion, insurance coverage is pivotal in reducing out-of-pocket costs for PBRT, transforming it from a financial burden into a viable treatment option. By understanding their policies, leveraging financial assistance, and advocating for broader coverage, patients can navigate the system more effectively. As insurers increasingly recognize the clinical and economic advantages of PBRT, its acceptance as a standard therapy will likely expand, benefiting thousands of breast cancer survivors annually. This shift underscores the interconnectedness of healthcare financing, treatment innovation, and patient empowerment in shaping accessible, affordable care.
Understanding Illinois' Definition of Life Insurance Replacement
You may want to see also
Explore related products

$9.59 $16.99




![]()
Clinical Evidence Impact: Strong clinical data supports insurance acceptance, driving broader coverage for partial breast radiation
The landscape of breast cancer treatment has evolved significantly, with partial breast radiation therapy (PBRT) emerging as a focal point of clinical research and insurance policy debates. Strong clinical evidence now underscores the efficacy and safety of PBRT, particularly for early-stage breast cancer patients aged 50 and older. Studies like the NSABP B-39 trial demonstrate that PBRT delivers comparable tumor control rates to whole breast radiation, with a 5-year local recurrence rate of 4.6% versus 4.1% for whole breast irradiation. This data has been pivotal in shifting insurer perspectives, as evidenced by Medicare’s 2020 coverage determination for PBRT, which followed the publication of long-term outcomes in *The New England Journal of Medicine*.
Analyzing the impact of clinical trials reveals a clear trend: insurers prioritize treatments backed by robust, peer-reviewed evidence. For instance, the American Society for Radiation Oncology (ASTRO) guidelines, updated in 2022, recommend PBRT as a standard option for eligible patients, citing its reduced treatment duration (3-5 days vs. 3-6 weeks for whole breast radiation) and lower toxicity profiles. Insurers such as UnitedHealthcare and Aetna have since expanded coverage, often requiring patients to meet specific criteria, such as tumor size ≤3 cm and negative lymph nodes. This alignment between clinical evidence and coverage policies highlights the power of data in driving healthcare access.
From a practical standpoint, providers can leverage this evidence to advocate for PBRT coverage on behalf of patients. Key steps include documenting patient eligibility based on tumor characteristics, age, and comorbidities, as well as referencing landmark trials like the TARGIT-A study, which showed non-inferiority of PBRT in 10-year outcomes. Additionally, emphasizing the cost-effectiveness of PBRT—estimated to reduce treatment costs by 30-50% compared to whole breast radiation—can further strengthen appeals to insurers. For patients, understanding these criteria and discussing them with their care team can expedite approval processes.
A comparative analysis of PBRT’s adoption across regions reveals disparities tied to insurance acceptance. In states where Medicare coverage has been widely publicized, such as Florida and California, PBRT utilization has increased by 25% since 2020. Conversely, in states with limited insurer acceptance, adoption remains stagnant. This underscores the need for continued advocacy and education, particularly in underserved areas. Providers can play a critical role by participating in multicenter trials and publishing institution-specific outcomes to bolster local coverage decisions.
In conclusion, the interplay between clinical evidence and insurance acceptance has been transformative for PBRT. As more insurers recognize its benefits, patients gain access to a treatment that balances efficacy with convenience and reduced side effects. For clinicians, staying abreast of evolving guidelines and actively engaging with payers ensures that evidence-based care remains within reach for all eligible patients. This dynamic exemplifies how strong data not only advances medical practice but also shapes healthcare policy.
Understanding Life Insurance: Surrender Charges Explained
You may want to see also
Frequently asked questions
Yes, partial breast radiation therapy (PBRT) is increasingly accepted and covered by most insurance plans, including Medicare and many private insurers, as it is a recognized and effective treatment option for early-stage breast cancer.
Coverage depends on the specific insurance plan, the patient’s medical history, and whether the treatment aligns with established clinical guidelines. Pre-authorization may be required, and coverage varies by provider.
While most major insurers cover PBRT, some smaller or regional plans may have restrictions or exclude it. Patients should verify coverage with their insurance provider and healthcare team.
Yes, Medicare typically covers partial breast radiation therapy when it is deemed medically necessary and meets the criteria for early-stage breast cancer treatment. Coverage may vary based on the specific Medicare plan.