Health insurance coverage for cholinesterase inhibitors, a class of medications commonly prescribed for conditions like Alzheimer’s disease and other forms of dementia, varies widely depending on the insurance provider, plan type, and specific policy details. These medications, which include drugs like donepezil, rivastigmine, and galantamine, are often considered essential for managing cognitive decline, but their cost can be a significant burden for patients and caregivers. Most private insurance plans and Medicare Part D prescription drug plans typically cover cholinesterase inhibitors, though coverage may be subject to prior authorization, step therapy, or tiered copayments. Medicaid coverage also varies by state, with some states offering more comprehensive benefits than others. Patients and caregivers should carefully review their insurance policies or consult with their provider to understand the extent of coverage and any out-of-pocket expenses associated with these medications.
| Characteristics | Values |
|---|---|
| Coverage by Health Insurance | Varies by plan and insurer. Many private insurance plans, Medicare Part D, and some Medicaid plans cover cholinesterase inhibitors, but coverage may depend on the specific drug, diagnosis, and prior authorization requirements. |
| Commonly Covered Conditions | Alzheimer's disease, Parkinson's disease dementia, and other forms of dementia where cholinesterase inhibitors are clinically indicated. |
| Drugs Typically Covered | Donepezil (Aricept), Rivastigmine (Exelon), Galantamine (Razadyne), and Tacrine (Cognex), though Tacrine is less commonly prescribed due to side effects. |
| Prior Authorization | Often required. Insurers may mandate documentation of diagnosis, trial of therapy, and regular monitoring to ensure continued coverage. |
| Tier Placement | Typically placed in higher tiers (Tier 3 or 4) in prescription drug formularies, resulting in higher out-of-pocket costs for patients. |
| Cost-Sharing | Copays, coinsurance, or deductibles apply. Costs vary widely based on insurance plan, pharmacy, and whether generic or brand-name drugs are used. |
| Medicare Part D Coverage | Covered under Part D prescription drug plans, but coverage and costs depend on the specific plan and formulary. |
| Medicaid Coverage | Coverage varies by state. Some states cover cholinesterase inhibitors under Medicaid, but restrictions may apply. |
| Generic Availability | Generic versions of donepezil, rivastigmine, and galantamine are available, which can reduce costs compared to brand-name options. |
| Patient Assistance Programs | Available for some brand-name drugs (e.g., Aricept, Exelon) to help eligible patients with out-of-pocket costs. |
| Coverage Denials | Possible if the insurer deems the drug not medically necessary or if prior authorization criteria are not met. Appeals processes are available. |
| Formulary Changes | Coverage may change annually as insurers update their formularies. Patients should review their plan details each year. |
| Off-Label Use Coverage | Less likely to be covered if used off-label (e.g., for conditions other than approved indications). |
| Monitoring Requirements | Insurers may require periodic reassessment of the patient's condition to continue coverage. |
Explore related products






What You'll Learn
![]()
Coverage for Alzheimer’s treatment
Cholinesterase inhibitors are a cornerstone of Alzheimer's disease management, yet their coverage under health insurance plans varies widely. These medications, including donepezil (Aricept), rivastigmine (Exelon), and galantamine (Razadyne), work by increasing acetylcholine levels in the brain, which can temporarily improve cognitive function and slow symptom progression. For patients and caregivers, understanding insurance coverage is critical, as these drugs can cost upwards of $300 per month without assistance. Most Medicare Part D plans and private insurers cover cholinesterase inhibitors, but prior authorization or step therapy requirements often complicate access. Patients may need to try a generic version first or provide documentation of Alzheimer’s diagnosis to qualify for coverage.
Analyzing the nuances of insurance policies reveals a patchwork of coverage that can leave some patients underserved. While Medicare Part D typically includes cholinesterase inhibitors in its formulary, the specific tier placement affects out-of-pocket costs. For instance, donepezil, available in generic form, is often on lower tiers with copays as low as $10, whereas brand-name options like Exelon Patch may require coinsurance of 25% or more. Private insurance plans vary further, with some employers offering comprehensive drug coverage and others limiting access through high deductibles or exclusions for certain medications. Medicaid coverage differs by state, with some programs providing robust access and others imposing strict eligibility criteria for Alzheimer’s treatments.
For caregivers navigating this landscape, proactive steps can streamline access to cholinesterase inhibitors. Start by reviewing the insurance plan’s drug formulary to confirm coverage and tier placement. If the medication is not covered, request a formulary exception or appeal the decision with a physician’s support. Patient assistance programs, such as those offered by pharmaceutical companies, can provide financial aid for uninsured or underinsured individuals. For example, the Aricept Patient Assistance Program offers free medication to eligible low-income patients. Additionally, organizations like the Alzheimer’s Foundation of America offer resources to help families understand their insurance benefits and explore alternative funding options.
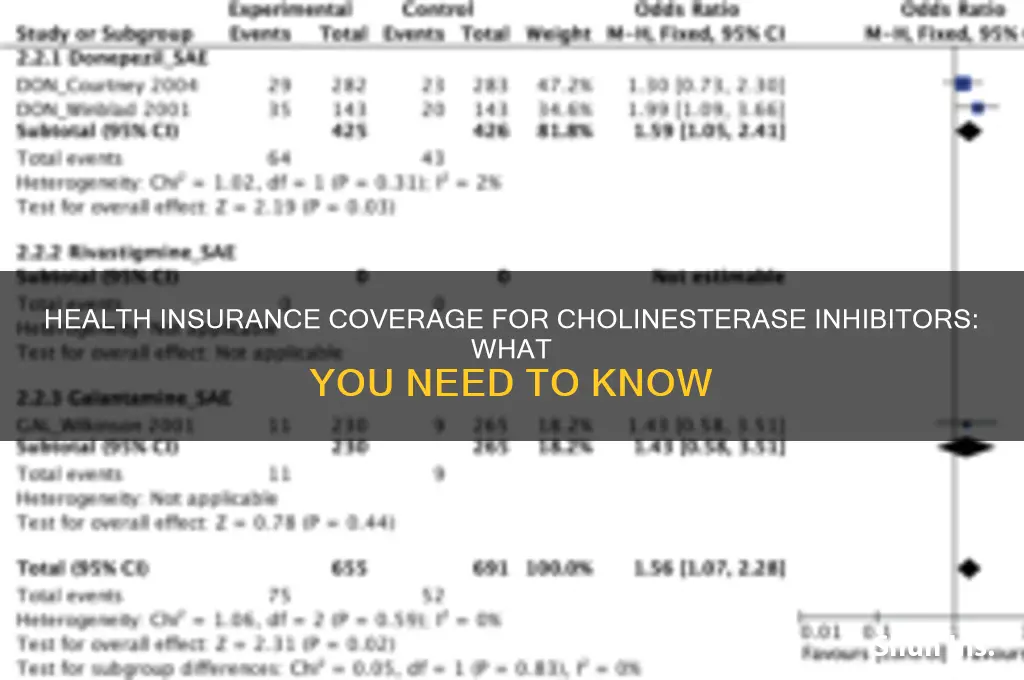
Comparing cholinesterase inhibitors to other Alzheimer’s treatments highlights the importance of insurance coverage in shaping treatment decisions. While these drugs are the most widely prescribed, newer therapies like aducanumab (Aduhelm) present a different coverage challenge due to their high cost and limited clinical benefit. Insurers often restrict access to aducanumab, requiring extensive documentation and prior authorization, whereas cholinesterase inhibitors face fewer barriers. However, the modest efficacy of cholinesterase inhibitors—improving symptoms by 6–12 months on average—means they are often the first-line treatment, making their affordability a priority for patients in the early to moderate stages of Alzheimer’s.
In conclusion, securing coverage for cholinesterase inhibitors requires a combination of advocacy, research, and strategic planning. Patients and caregivers must familiarize themselves with their insurance plan’s specifics, leverage available resources, and be prepared to appeal denials. While these medications are not a cure, their role in managing Alzheimer’s symptoms underscores the need for equitable access. As the prevalence of Alzheimer’s continues to rise, insurers and policymakers must prioritize coverage for these essential treatments to support the millions of individuals and families affected by the disease.
Medical Membership Insurance: Understanding the Cost of Coverage
You may want to see also
Explore related products



$35.24 $37.99
$15.88 $28.99


![]()
Medicare/Medicaid policies on inhibitors
Medicare and Medicaid policies on cholinesterase inhibitors are pivotal for patients with Alzheimer’s disease or other dementias, as these medications (e.g., donepezil, rivastigmine, galantamine) are often the first line of treatment. Medicare Part D, which covers prescription drugs, typically includes these inhibitors in its formulary, but coverage varies by plan. Patients must navigate tiers of cost-sharing, with generic versions often costing less than brand-name options. Medicaid, on the other hand, is state-specific, and while it generally covers these medications, eligibility and copay requirements differ widely. For instance, some states require prior authorization or step therapy, where patients must try a preferred drug before others are covered.
Understanding the nuances of Medicare Part D is critical for maximizing coverage. Plans categorize drugs into tiers, with cholinesterase inhibitors often falling into Tier 2 or 3, meaning moderate out-of-pocket costs. Patients can use Medicare’s Plan Finder tool to compare formularies and estimated costs. For example, a 30-day supply of generic donepezil (23 mg) might cost $10-$30, while brand-name Aricept could exceed $500 without coverage. Beneficiaries should also consider plans with low deductibles or those offering additional coverage in the coverage gap (the "donut hole"). Practical tip: Enroll during the Annual Enrollment Period (October 15–December 7) to ensure the chosen plan aligns with your medication needs.
Medicaid’s role in covering cholinesterase inhibitors is more complex due to its state-administered nature. In states with expanded Medicaid, low-income seniors and disabled individuals are more likely to qualify for coverage. However, some states impose restrictions, such as limiting the number of prescriptions per month or requiring documentation of disease progression. For example, a patient in Texas might need a physician’s statement confirming moderate to severe Alzheimer’s before Medicaid approves coverage for galantamine. Patients and caregivers should consult their state’s Medicaid handbook or contact a caseworker to understand specific requirements and appeal processes if coverage is denied.
A comparative analysis reveals that while both Medicare and Medicaid cover cholinesterase inhibitors, Medicare Part D offers more standardized access, whereas Medicaid’s variability can create barriers. For instance, Medicare’s nationwide structure ensures consistency in drug availability, whereas Medicaid’s state-by-state approach may leave some patients with limited options. Additionally, Medicare Advantage plans often bundle Part D coverage with additional benefits, such as care coordination for dementia patients, which can be advantageous. In contrast, Medicaid’s broader eligibility for low-income individuals makes it a lifeline for those who cannot afford Medicare premiums or copays.
To navigate these policies effectively, patients and caregivers should take proactive steps. First, verify the specific cholinesterase inhibitor prescribed and check its coverage under your Medicare Part D plan or Medicaid formulary. Second, explore patient assistance programs offered by pharmaceutical companies, which can reduce costs for brand-name medications. Third, consider consulting a pharmacist or social worker to identify gaps in coverage and potential solutions. Finally, stay informed about policy changes, as updates to Medicare or Medicaid guidelines can impact access to these critical medications. By combining knowledge of these policies with practical strategies, patients can optimize their coverage and manage dementia treatment more effectively.
Understanding Medicare Enrollment: When to Sign Up
You may want to see also
Explore related products






![]()
Private insurance limitations
Private insurance coverage for cholinesterase inhibitors often hinges on the diagnosis and stage of the condition being treated. For instance, these medications are primarily prescribed for mild to moderate Alzheimer’s disease, but insurers may require documented cognitive testing, such as the Mini-Mental State Examination (MMSE), to confirm eligibility. If a patient scores below 10 on the MMSE, coverage might be denied under the assumption that the medication’s benefits are minimal at advanced stages. This diagnostic threshold creates a narrow window for patients to access treatment, leaving those in early or late stages potentially uncovered.
Another limitation arises from the tiered formulary systems used by private insurers. Cholinesterase inhibitors like donepezil (Aricept), rivastigmine (Exelon), and galantamine (Razadyne) are often placed in higher tiers, requiring patients to pay a larger copay or coinsurance. For example, a 30-day supply of brand-name donepezil 10 mg could cost $150 out-of-pocket compared to $10 for a preferred generic. Insurers may also mandate step therapy, requiring patients to fail on a cheaper generic before approving a more expensive option, even if the prescribing physician deems it less suitable.
Prior authorization is a common barrier that delays or prevents access to cholinesterase inhibitors. Insurers typically require detailed documentation, including the patient’s diagnosis, previous treatments, and expected outcomes. This process can take weeks, during which patients may experience disease progression. For caregivers managing a loved one’s care, navigating these administrative hurdles adds stress and complexity, often leading to treatment abandonment. A 2020 study found that 30% of prior authorization requests for Alzheimer’s medications were initially denied, with 60% of those eventually approved after appeal—a process few families pursue.
Finally, private insurance plans often impose quantity limits on cholinesterase inhibitors, restricting the number of pills dispensed per prescription fill. For example, a plan might cover only 30 tablets per month, even if the prescribed dose is 23 mg daily (requiring 60 tablets). Patients must then request additional approvals or pay out-of-pocket for the remainder. This limitation disproportionately affects those on higher doses, such as donepezil 23 mg, which is often prescribed as disease progression necessitates increased dosage. Such restrictions undermine adherence, as patients may skip doses or ration medication to make it last until the next refill.
Top Medical Insurance Companies: Your Comprehensive Guide
You may want to see also
Explore related products






![]()
Out-of-pocket costs for inhibitors
Cholinesterase inhibitors, commonly prescribed for conditions like Alzheimer's disease, can significantly impact out-of-pocket costs for patients, even with insurance coverage. These medications, including donepezil, rivastigmine, and galantamine, are often essential for managing cognitive decline, but their financial burden varies widely depending on insurance plans, dosage requirements, and formulary placement. Understanding these factors is crucial for patients and caregivers navigating the complexities of medication affordability.
For instance, a standard dose of donepezil (10 mg daily) can cost uninsured patients upwards of $300 per month, while those with insurance may pay as little as $10 to $50 in copays. However, not all plans cover all inhibitors equally. Some insurers place these drugs in higher tiers, requiring patients to meet deductibles or pay coinsurance rates that can exceed 25% of the drug’s cost. For older adults on fixed incomes, these expenses can quickly become unsustainable, especially when combined with other healthcare needs.
To mitigate out-of-pocket costs, patients should first review their insurance plan’s drug formulary to understand coverage tiers and prior authorization requirements. Generic versions of inhibitors, such as donepezil, are often more affordable than brand-name alternatives like Aricept. Additionally, patient assistance programs offered by pharmaceutical companies or nonprofit organizations can provide financial relief for eligible individuals. For example, the Pfizer RxPathways program offers donepezil at reduced costs for those meeting income criteria.
Another practical strategy is to discuss dosage adjustments with a healthcare provider. In some cases, starting with a lower dose (e.g., 5 mg daily for donepezil) and titrating upward can reduce monthly expenses while still providing therapeutic benefits. Pharmacists can also help identify cost-saving opportunities, such as using 90-day supplies or mail-order pharmacies, which often offer lower copays than retail pharmacies.
Ultimately, while cholinesterase inhibitors are vital for many patients, their out-of-pocket costs demand proactive management. By leveraging insurance benefits, exploring assistance programs, and optimizing treatment plans, individuals can balance medical necessity with financial feasibility. Caregivers and patients alike should approach this challenge with a combination of research, advocacy, and collaboration with healthcare providers.
Medical Bills: Why Insurance Isn't Enough
You may want to see also
Explore related products





![]()
Pre-authorization requirements
Health insurance coverage for cholinesterase inhibitors often hinges on pre-authorization requirements, a critical step that can determine whether a patient receives these medications. Pre-authorization, also known as prior authorization, is a process where insurers review a prescription to ensure it meets specific criteria before approving coverage. For cholinesterase inhibitors, commonly prescribed for conditions like Alzheimer’s disease, this process typically involves verifying the diagnosis, assessing the patient’s medical history, and confirming that the medication is the most appropriate treatment option. Without pre-authorization, patients may face denials or delays in accessing these costly but essential drugs.
The pre-authorization process for cholinesterase inhibitors varies by insurer but generally requires detailed documentation from the prescribing physician. This includes a confirmed diagnosis of mild to moderate Alzheimer’s disease, evidence of cognitive decline, and often a trial of non-pharmacological interventions. For example, insurers may require proof that the patient has undergone cognitive testing, such as the Mini-Mental State Examination (MMSE), with scores typically ranging between 10 and 26 indicating eligibility. Additionally, some plans mandate that patients start with lower dosages, such as 5 mg daily for donepezil, before escalating to higher doses like 10 mg or 23 mg, to demonstrate tolerance and potential benefit.
One of the challenges with pre-authorization is the administrative burden it places on healthcare providers and patients. Physicians must submit detailed forms, often including treatment plans, lab results, and progress notes, which can delay treatment initiation. For patients, this delay can be particularly detrimental, as timely intervention with cholinesterase inhibitors is crucial for managing symptoms and slowing disease progression. To streamline this process, providers can proactively include all required documentation in their initial submission and follow up with insurers to ensure timely review. Patients or caregivers should also familiarize themselves with their insurance plan’s specific requirements, as some may allow appeals if coverage is initially denied.
Comparatively, pre-authorization requirements for cholinesterase inhibitors are often stricter than those for other medications due to their high cost and specific indications. For instance, while a generic antibiotic might require minimal review, cholinesterase inhibitors like rivastigmine or galantamine often necessitate periodic reauthorization, typically every 6 to 12 months, to ensure continued medical necessity. This ongoing scrutiny reflects insurers’ efforts to balance access to effective treatments with cost management. Patients and providers can advocate for smoother approvals by highlighting the medication’s potential to reduce caregiver burden and delay institutionalization, which can offset long-term healthcare costs.
In conclusion, navigating pre-authorization requirements for cholinesterase inhibitors demands proactive communication, thorough documentation, and an understanding of insurer-specific criteria. By preparing in advance and staying informed, patients and providers can minimize delays and improve access to these vital medications. For those facing repeated denials, consulting a pharmacist or utilizing patient assistance programs offered by pharmaceutical companies may provide additional pathways to coverage. Ultimately, while pre-authorization can be a hurdle, it is a navigable one with the right approach.
Carondelet Medical Group: Accepted Insurance Plans and Policies
You may want to see also
Frequently asked questions
Yes, most health insurance plans, including Medicare and private insurers, cover cholinesterase inhibitors, as they are FDA-approved medications for conditions like Alzheimer’s disease. However, coverage may vary based on the specific plan, formulary, and prior authorization requirements.
Out-of-pocket costs depend on your insurance plan. Some plans may require copays, coinsurance, or deductibles. Generic versions of these medications are often more affordable, while brand-name options may have higher costs.
If coverage is denied, you can appeal the decision with your insurance provider. Your healthcare provider can assist by submitting additional documentation or requesting a formulary exception. Patient assistance programs or manufacturer discounts may also be available to reduce costs.




























