The rise of insurance as a dominant force in healthcare has fundamentally transformed the industry, often to its detriment. Initially intended to protect individuals from catastrophic medical expenses, insurance has instead created a complex, profit-driven system that prioritizes administrative costs and shareholder returns over patient care. By inserting intermediaries between providers and patients, insurance companies have inflated prices, incentivized unnecessary treatments, and stifled competition, leading to a bloated and inefficient healthcare system. This dynamic has shifted the focus from preventive care and patient outcomes to billing codes and coverage limitations, leaving many Americans with skyrocketing premiums, high deductibles, and limited access to affordable, quality care. As a result, what was once a system designed to safeguard health has become a barrier to it, raising critical questions about the role of insurance in modern healthcare.
| Characteristics | Values |
|---|---|
| Increased Administrative Costs | Insurance companies add significant administrative overhead, with estimates suggesting 25-30% of healthcare costs going to billing and insurance-related paperwork (Source: Health Affairs, 2023). |
| Reduced Price Transparency | Insurance-driven pricing obscures actual costs, making it difficult for patients to compare prices or negotiate, leading to higher overall spending (Source: JAMA, 2022). |
| Overutilization of Services | Fee-for-service models incentivize providers to order more tests and procedures, often unnecessary, to maximize reimbursement (Source: NEJM, 2021). |
| Narrow Networks | Insurance plans limit provider choices, reducing patient access to preferred doctors and specialists, often to cut costs (Source: Kaiser Family Foundation, 2023). |
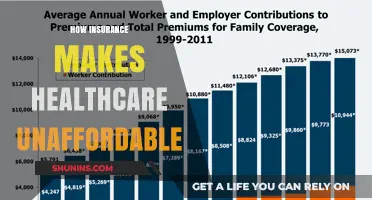
| High Premiums and Deductibles | Rising insurance premiums and deductibles shift more financial burden onto patients, leading to delayed or forgone care (Source: Commonwealth Fund, 2023). |
| Prior Authorization Delays | Insurance requirements for prior authorization cause delays in treatment, potentially worsening patient outcomes (Source: AMA, 2022). |
| Provider Burnout | The complexity of dealing with multiple insurance plans and claims contributes to physician burnout and reduced quality of care (Source: Mayo Clinic Proceedings, 2023). |
| Profit-Driven Decisions | Insurance companies prioritize profit over patient care, often denying claims or coverage for necessary treatments (Source: Public Citizen, 2022). |
| Fragmented Care | Insurance-driven systems create fragmented care, with poor coordination between providers, leading to inefficiencies and errors (Source: Annals of Internal Medicine, 2021). |
| Reduced Preventive Care | High out-of-pocket costs discourage patients from seeking preventive care, leading to more costly treatments later (Source: CDC, 2023). |
Explore related products






What You'll Learn
- Excessive Administrative Costs: Insurance bureaucracy increases overhead, diverting funds from patient care to paperwork
- Fee-for-Service Incentives: Encourages unnecessary treatments, prioritizing profit over patient health and outcomes
- Narrow Networks: Limits provider choices, reducing access to quality care and increasing out-of-pocket costs
- Prior Authorization Delays: Insurers stall approvals, delaying critical treatments and worsening patient conditions
- Profit-Driven Denials: Claims are often denied to maximize profits, leaving patients vulnerable and uninsured
![]()
Excessive Administrative Costs: Insurance bureaucracy increases overhead, diverting funds from patient care to paperwork
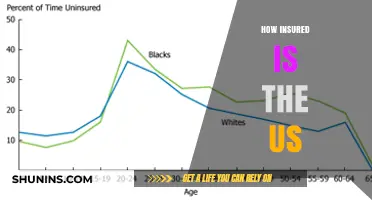
The U.S. healthcare system spends nearly $1 trillion annually on administrative costs, with insurance bureaucracy accounting for a significant portion. To put this in perspective, this amount could fund the entire annual budget of the U.S. Department of Defense, yet it yields no direct patient care. Instead, it fuels a labyrinthine system of claims processing, prior authorizations, and billing disputes. For every dollar spent on healthcare, nearly 30 cents goes toward administrative overhead, compared to single-payer systems like Canada’s, where the figure hovers around 12 cents. This disparity underscores how insurance bureaucracy diverts resources from where they’re most needed: patient care.
Consider the daily workflow of a primary care physician. On average, they spend nearly 6 hours per week navigating prior authorization requirements alone—time that could be allocated to patient consultations. A 2021 study by the American Medical Association found that 94% of physicians reported care delays due to insurance red tape, with 33% noting these delays led to serious adverse events. For patients, this translates to longer wait times, fragmented care, and increased frustration. Meanwhile, hospitals and clinics employ armies of billing specialists to decipher complex insurance policies, negotiate claims, and rectify payment errors. These roles, while necessary in the current system, siphon funds that could otherwise finance additional nursing staff, updated medical equipment, or reduced out-of-pocket costs for patients.
To illustrate, let’s examine a common scenario: a patient with diabetes requires a new glucose monitor. The process begins with the physician submitting a prior authorization request, which takes an average of 8 days to approve—during which the patient’s condition may worsen. The device itself costs $200, but the administrative effort to secure approval adds an estimated $50 in hidden costs. Multiply this by thousands of similar cases daily, and the inefficiency becomes systemic. Insurance companies argue these steps prevent fraud and ensure appropriate care, but the evidence suggests the opposite: a 2018 JAMA study found that only 1.5% of denied claims were overturned on appeal, indicating that most rejections are unnecessary barriers rather than safeguards.
Reducing administrative bloat requires systemic reform, but incremental steps can yield immediate benefits. For instance, standardizing prior authorization forms across insurers could save providers up to 15 hours per week, according to the AMA. Policymakers could mandate transparency in administrative spending, requiring insurers to publicly report the percentage of premiums allocated to overhead versus patient care. Employers, who often foot the bill for health plans, could negotiate contracts prioritizing low-bureaucracy insurers. Patients can advocate for themselves by scrutinizing Explanation of Benefits statements for errors—a 2020 study found that 80% of medical bills contain inaccuracies, often inflating costs unnecessarily.
Ultimately, the administrative burden of insurance is not an inevitable feature of healthcare but a design flaw. Every dollar spent on paperwork is a dollar not spent on vaccines, mental health services, or chronic disease management. Until stakeholders—insurers, providers, and policymakers—prioritize streamlining bureaucracy, the system will continue to hemorrhage resources, leaving patients to bear the cost in both dollars and health outcomes. The question isn’t whether reform is possible, but whether the will to challenge entrenched inefficiencies exists.
Securing Your Exodus-Held EOS: Eligibility and Insurance Tips
You may want to see also
Explore related products

$11.49 $19.99





![]()
Fee-for-Service Incentives: Encourages unnecessary treatments, prioritizing profit over patient health and outcomes
The fee-for-service (FFS) model, a cornerstone of healthcare reimbursement, inherently rewards quantity over quality. Under this system, providers are paid for each service rendered—every test, procedure, and consultation. This structure creates a perverse incentive: the more interventions, the higher the revenue. For instance, a study published in the *Journal of the American Medical Association* found that physicians in FFS systems ordered 25% more imaging tests than their counterparts in salaried or capitated models, even when patient outcomes did not improve. This overutilization not only inflates healthcare costs but also exposes patients to unnecessary risks, such as radiation from repeated CT scans or complications from invasive procedures.
Consider a 65-year-old patient with chronic back pain. In an FFS system, a provider might recommend a series of expensive MRI scans, physical therapy sessions, and even spinal injections—all billable services. While some of these interventions may offer marginal relief, the cumulative cost to the patient and the system is staggering. In contrast, a value-based care model might prioritize a single, comprehensive assessment followed by targeted, evidence-based treatments, reducing both expense and patient burden. The FFS model, however, lacks this restraint, as financial incentives align with maximizing services rather than optimizing outcomes.
To illustrate the practical implications, imagine a primary care physician with a full schedule. Under FFS, there’s a financial disincentive to spend extra time counseling a patient on lifestyle changes, such as diet and exercise, which could prevent future health issues. Instead, the physician might quickly order lab tests or refer the patient to a specialist, ensuring a higher reimbursement. This short-term focus on revenue undermines long-term patient health, perpetuating a cycle of dependency on medical interventions rather than preventive care.
Breaking free from this model requires systemic change. One approach is transitioning to value-based care, where providers are paid based on patient outcomes rather than the volume of services. For example, bundled payments for episodes of care, such as joint replacements, incentivize efficiency and quality. Additionally, patients can advocate for themselves by questioning the necessity of tests or procedures, requesting evidence-based alternatives, and seeking providers who prioritize preventive care. Policymakers also play a role by implementing regulations that penalize overutilization and reward coordinated, patient-centered care.
Ultimately, the FFS model’s emphasis on profit over patient health is a symptom of a broader misalignment in healthcare incentives. By recognizing this flaw and adopting alternative payment structures, the system can shift toward a more sustainable, patient-focused approach. Until then, both providers and patients must navigate a landscape where financial motives often overshadow clinical judgment, perpetuating a cycle of unnecessary treatments and escalating costs.
Estimating Umbrella Insurance: A Step-by-Step Guide to Adequate Coverage
You may want to see also
Explore related products






![]()
Narrow Networks: Limits provider choices, reducing access to quality care and increasing out-of-pocket costs
Narrow networks, a cost-cutting strategy employed by insurance companies, restrict patients to a limited list of healthcare providers within their plan. This seemingly innocuous tactic has far-reaching consequences, ultimately undermining the very essence of healthcare: access to quality care. Imagine being diagnosed with a complex condition, only to discover that the specialist with the most experience treating it is excluded from your network, leaving you with limited options and potentially compromising your treatment outcomes.
This scenario is not merely hypothetical; it's a stark reality for millions of Americans. A 2019 study by the Kaiser Family Foundation found that 45% of large employer-sponsored plans utilized narrow networks, effectively limiting patient choice and access to preferred providers.
The impact of narrow networks extends beyond inconvenience. By restricting access to specialists and renowned medical centers, these networks can delay diagnoses, hinder treatment options, and ultimately lead to poorer health outcomes. Consider a patient with a rare autoimmune disease. A narrow network might exclude the few specialists in the region with expertise in this condition, forcing the patient to settle for a general practitioner with limited experience, potentially leading to misdiagnosis or inadequate treatment.
Moreover, narrow networks often push patients towards in-network providers who may be less experienced or have lower patient satisfaction ratings. This can result in a frustrating and potentially detrimental healthcare experience, leaving patients feeling disempowered and dissatisfied.
The financial burden of narrow networks is equally concerning. While these networks are marketed as cost-saving measures, they often shift the financial burden onto patients. Out-of-network care, even when medically necessary, can result in exorbitant out-of-pocket expenses, leaving patients facing difficult choices between their health and their financial well-being. For instance, a patient requiring a specific surgical procedure performed by an out-of-network surgeon might face bills exceeding tens of thousands of dollars, despite having insurance coverage.
The solution to the narrow network dilemma lies in increased transparency and patient empowerment. Consumers must demand greater clarity from insurance companies regarding network limitations and potential out-of-pocket costs. Policymakers should implement regulations that ensure adequate network breadth and accessibility, particularly for specialists and geographically underserved areas. Ultimately, healthcare should prioritize patient needs over profit margins, ensuring that everyone has access to the care they need, when they need it, without facing financial ruin.
Borrowing Against Your MBA Life Insurance: Is it Possible?
You may want to see also
Explore related products






![]()
Prior Authorization Delays: Insurers stall approvals, delaying critical treatments and worsening patient conditions
Prior authorization delays have become a silent epidemic in healthcare, turning insurers into gatekeepers who prioritize profit over patient well-being. Consider a 62-year-old woman diagnosed with metastatic breast cancer. Her oncologist prescribes a targeted therapy, palbociclov 125 mg daily, proven to slow tumor growth and extend survival. Yet, her insurer flags the $15,000 monthly cost, requiring prior authorization. What should be a 48-hour approval process stretches into three weeks of back-and-forth faxes, denials, and appeals. During this delay, her cancer progresses, shrinking her treatment window and worsening her prognosis. This isn’t an anomaly—it’s a systemic issue. A 2021 AMA survey found 94% of physicians reported prior authorization delays led to adverse patient outcomes, from disease progression to hospitalization. Insurers argue this process curbs unnecessary spending, but the evidence suggests it’s a stalling tactic to avoid covering expensive, life-saving treatments.
To understand the mechanics of this delay, imagine a labyrinth designed to frustrate both patients and providers. Step one: The physician submits a prior authorization request, often through a clunky online portal or fax system. Step two: The insurer reviews the request, frequently denying it for vague reasons like “lack of medical necessity” or “non-formulary drug.” Step three: The physician appeals, providing additional documentation, such as lab results or imaging reports. Step four: The insurer may approve, deny again, or request further information, restarting the cycle. This process, which can take days to months, is particularly devastating for patients needing urgent care. For instance, a 45-year-old man with severe plaque psoriasis prescribed a biologic like adalimumab 40 mg every other week may face a denial because the insurer insists on a cheaper, less effective alternative. By the time the appeal succeeds, his skin lesions have worsened, and he’s developed joint pain from psoriatic arthritis—a complication that could have been prevented with timely treatment.
The human cost of these delays is immeasurable, but the financial implications are clear: Insurers save billions by delaying or denying coverage for high-cost medications and procedures. Take the case of a 55-year-old diabetic patient prescribed a continuous glucose monitor (CGM) to manage his blood sugar levels. The CGM costs $1,000 upfront but prevents costly ER visits and long-term complications like kidney failure. Yet, his insurer denies the request, claiming it’s “not medically necessary.” After a month-long appeal, the patient’s A1C rises from 7.5% to 9.2%, increasing his risk of diabetic retinopathy and neuropathy. The insurer avoids the $1,000 expense but shifts the burden to the patient and the healthcare system, which will eventually bear the $30,000 cost of dialysis or amputation. This perverse incentive structure rewards insurers for delaying care, turning prior authorization into a weapon against patients.
Patients and providers aren’t powerless in this battle. Practical steps can mitigate the impact of prior authorization delays. First, physicians should document every interaction with insurers, including dates, names, and denial reasons. This creates a paper trail for appeals and potential legal action. Second, patients should advocate for themselves by contacting their insurer’s patient advocate or filing a complaint with their state’s insurance commissioner. Third, providers can use technology to streamline the prior authorization process. Software like CoverMyMeds automates requests, reducing the administrative burden and speeding up approvals. Finally, policymakers must act. Legislation like the Improving Seniors’ Timely Access to Care Act aims to standardize and expedite prior authorization for Medicare Advantage plans. While not a cure-all, these measures can chip away at the bureaucratic barriers insurers erect, restoring the focus of healthcare to where it belongs: the patient.
Insurance Documents as Proof of Residency: What You Need to Know
You may want to see also
Explore related products






![]()
Profit-Driven Denials: Claims are often denied to maximize profits, leaving patients vulnerable and uninsured
Insurance companies, driven by profit motives, have mastered the art of claim denial, leaving patients in a precarious position. Consider this: a 45-year-old woman with a history of chronic migraines is prescribed a new medication, only to have her claim denied due to a technicality in her policy. The insurer cites a pre-existing condition clause, despite her condition being well-managed for years. This scenario is not uncommon, as insurers often employ tactics to minimize payouts, prioritizing shareholders' returns over policyholders' well-being.
To understand the mechanics of profit-driven denials, let's examine the claims review process. Insurers use complex algorithms and human reviewers to assess claims, but the criteria are often skewed in their favor. For instance, a claim for a high-cost procedure like a knee replacement might be denied if the patient's body mass index (BMI) exceeds a certain threshold, even if the procedure is medically necessary. This approach allows insurers to avoid costly payouts while maintaining a veneer of legitimacy. A 2020 study found that 1 in 5 claims submitted to private insurers were initially denied, with patients forced to navigate a complex appeals process to secure coverage.
The consequences of these denials can be devastating. Imagine a 62-year-old man with type 2 diabetes who requires a specific insulin brand to manage his condition. His insurer denies coverage for this brand, opting for a cheaper alternative that proves ineffective. As a result, his blood sugar levels fluctuate, leading to complications like neuropathy and vision problems. This example illustrates how profit-driven denials can compromise patient health, particularly among vulnerable populations. To mitigate these risks, patients should: (1) carefully review their policy documents, (2) maintain detailed medical records, and (3) seek assistance from patient advocacy groups when facing denials.
A comparative analysis of insurance practices in the United States and countries with universal healthcare systems reveals stark differences. In Canada, for instance, patients are less likely to face claim denials, as the system prioritizes access to care over profit. In contrast, the U.S. system, with its reliance on private insurers, creates a perverse incentive to deny claims. This disparity highlights the need for systemic reform, such as implementing stricter regulations on claim denial practices or exploring alternative models like a public option. By learning from other systems, we can work towards a healthcare model that prioritizes patient well-being over corporate profits.
Ultimately, addressing profit-driven denials requires a multifaceted approach. Policymakers must enact legislation that holds insurers accountable for unjust denials, while patients must become more informed advocates for their own care. For example, the implementation of a standardized claims review process, coupled with increased transparency in denial rates, could help curb abusive practices. Additionally, insurers should be required to provide clear, actionable guidance on how to appeal denials, ensuring that patients have a fair chance to secure the care they need. By taking these steps, we can begin to unravel the complex web of profit-driven denials and move towards a more just and equitable healthcare system.
Life Insurance: Many Unprotected, What's the Reason?
You may want to see also
Frequently asked questions
Insurance has driven up healthcare costs by creating a system where providers charge higher prices to offset negotiated discounts with insurers, while insurers pass these costs onto consumers through premiums and out-of-pocket expenses.
Insurance companies restrict patient choice by dictating which providers and treatments are covered through narrow networks and prior authorization requirements, prioritizing cost control over patient needs.
Insurance has incentivized healthcare providers to prioritize billing and administrative tasks over patient care, as reimbursement models reward quantity of services over quality of outcomes.