The issue of healthcare access in the United States remains a pressing concern, with millions of Americans still lacking health insurance coverage. Despite efforts to expand access through initiatives like the Affordable Care Act, a significant portion of the population continues to face barriers to obtaining essential medical care. Factors such as high insurance premiums, limited employer-sponsored plans, and gaps in public programs like Medicaid contribute to this persistent problem. Understanding the scope and demographics of the uninsured population is crucial for addressing disparities and developing effective solutions to ensure that all Americans have access to affordable and comprehensive healthcare.
Explore related products






What You'll Learn
![]()
Uninsured rate trends over time
The uninsured rate in the United States has seen significant fluctuations over the past few decades, shaped by policy changes, economic shifts, and societal trends. From the early 2000s to the mid-2010s, the uninsured rate hovered around 15%, with millions of Americans lacking access to healthcare coverage. The passage of the Affordable Care Act (ACA) in 2010 marked a turning point, introducing expansions in Medicaid and the establishment of health insurance marketplaces. By 2016, the uninsured rate had dropped to a historic low of 8.6%, reflecting the impact of these reforms. However, subsequent policy rollbacks and economic challenges have since influenced this trend, highlighting the dynamic nature of healthcare access in the U.S.
Analyzing the data reveals a clear pattern: policy decisions have a direct and immediate effect on uninsured rates. For instance, states that expanded Medicaid under the ACA saw steeper declines in uninsured populations compared to those that did not. In 2019, non-expansion states had an average uninsured rate of 13.7%, nearly double that of expansion states at 7.3%. This disparity underscores the importance of state-level decisions in shaping healthcare access. Additionally, demographic factors play a role; younger adults (ages 18–34) and low-income households remain disproportionately uninsured, often due to affordability concerns or lack of employer-sponsored coverage.
To understand the trajectory of uninsured rates, it’s essential to examine economic influences. During the Great Recession (2007–2009), the uninsured rate rose as job losses led to the loss of employer-based insurance. Conversely, economic recovery post-2010 contributed to the decline in uninsured rates, as more individuals gained employment with benefits. However, the COVID-19 pandemic introduced new challenges, with initial job losses threatening to reverse progress. Surprisingly, the uninsured rate remained relatively stable during this period, partly due to emergency measures like the continuous enrollment provision in Medicaid. This example illustrates how external crises can both disrupt and, in some cases, inadvertently stabilize healthcare coverage trends.
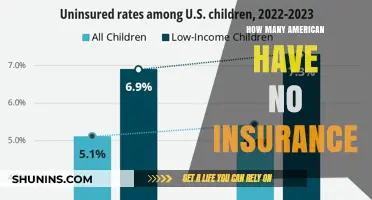
A comparative look at uninsured rates across age groups provides further insight. Children have consistently maintained lower uninsured rates, thanks to programs like the Children’s Health Insurance Program (CHIP). In 2022, only 4.6% of children were uninsured, compared to 12.9% of adults aged 19–64. This gap highlights the success of targeted policies for younger populations while revealing areas for improvement in adult coverage. Practical steps to address this include expanding Medicaid in non-expansion states and increasing subsidies for marketplace plans, which could significantly reduce uninsured rates among adults.
In conclusion, uninsured rate trends over time are a reflection of the interplay between policy, economics, and demographics. While progress has been made, particularly following the ACA, challenges remain in ensuring consistent and equitable access to healthcare. Policymakers, advocates, and individuals must remain vigilant in addressing gaps, especially among vulnerable populations. By learning from past trends and adapting strategies, the U.S. can continue to move toward a future where healthcare coverage is accessible to all.
Life Insurance Payouts: Are They Taxable Income?
You may want to see also
Explore related products






![]()
Reasons for lacking health insurance coverage
As of recent data, approximately 8.5% of Americans, or about 28 million people, lack health insurance coverage. This figure, while lower than pre-Affordable Care Act (ACA) levels, still highlights significant gaps in access to healthcare. Understanding the reasons behind this lack of coverage is crucial for addressing the issue effectively.
Economic Barriers: The Cost Conundrum
For many uninsured Americans, the primary obstacle is cost. Despite the ACA’s subsidies, premiums, deductibles, and out-of-pocket expenses remain prohibitively expensive for low-income individuals and families. For example, a 40-year-old earning $50,000 annually might face monthly premiums of $400 or more, coupled with a $4,000 deductible. Without employer-sponsored insurance, these costs often force individuals to choose between healthcare and basic necessities like rent or groceries. Even Medicaid, while a lifeline for millions, has gaps in states that have not expanded eligibility under the ACA, leaving an estimated 2.2 million people in the "coverage gap" earning too much for Medicaid but too little for marketplace subsidies.
Employment-Based Coverage Gaps
A significant portion of Americans rely on employer-sponsored insurance, yet not all jobs offer this benefit. Part-time workers, gig economy participants, and small business employees are particularly vulnerable. For instance, a freelance graphic designer or a part-time retail worker may not qualify for employer-provided insurance, leaving them to navigate the individual market. Even when offered, some employees decline coverage due to high employee contributions, a phenomenon more common in low-wage industries. This reliance on employment-based insurance creates a precarious situation where job loss or change can result in immediate loss of coverage.
Administrative and Systemic Hurdles
Navigating the complexities of the healthcare system can deter individuals from obtaining insurance. Enrollment processes, eligibility requirements, and frequent policy changes create barriers, especially for those with limited literacy or access to technology. For example, undocumented immigrants are ineligible for Medicaid or ACA marketplace plans, leaving them with few affordable options. Additionally, periodic enrollment windows and documentation requirements can exclude those who miss deadlines or lack necessary paperwork. These systemic challenges disproportionately affect marginalized communities, exacerbating disparities in coverage.
Personal Choices and Misinformation
While less common, some individuals forgo insurance due to personal choice or misinformation. Young, healthy adults may perceive themselves as low-risk and opt to pay the penalty (where applicable) rather than purchase coverage. Others may be misinformed about available subsidies or believe they cannot afford insurance without fully exploring their options. For instance, a 25-year-old might qualify for a $0 premium plan with cost-sharing reductions but remain uninsured due to lack of awareness. Addressing these gaps requires targeted education campaigns and simplified enrollment processes to ensure informed decision-making.
Policy and Political Factors
Finally, policy decisions play a significant role in insurance coverage rates. The ACA’s survival has been threatened by legal challenges and political opposition, creating uncertainty for consumers. Efforts to repeal or replace the law could strip millions of their coverage, particularly those with pre-existing conditions. Additionally, the lack of a universal healthcare system leaves the U.S. reliant on a patchwork of public and private programs, resulting in coverage gaps. Until systemic reforms address these underlying issues, millions will continue to face barriers to affordable, accessible healthcare.
By dissecting these reasons—economic, employment-related, administrative, personal, and political—policymakers and advocates can develop targeted solutions to reduce the number of uninsured Americans and move closer to universal coverage.
Does Social Security Affect Marketplace Insurance Income Eligibility?
You may want to see also
Explore related products






![]()
Impact of income on insurance status
Income is a decisive factor in determining whether Americans have health insurance, with lower-income individuals facing significantly higher uninsured rates. According to the U.S. Census Bureau, in 2022, 8.0% of Americans lacked health insurance, but this figure masks stark disparities: 13.3% of those in households earning below $25,000 annually were uninsured, compared to just 3.8% in households earning $100,000 or more. This gap highlights how financial constraints directly limit access to coverage, as lower-income families often cannot afford premiums, deductibles, or copays, even when subsidized options are available.
Consider the mechanics of this disparity: for a family of four earning $24,000 annually, the average annual premium for employer-sponsored health insurance (approximately $6,000) consumes nearly 25% of their income. Even with subsidies through the Affordable Care Act (ACA) marketplace, out-of-pocket costs remain prohibitive. For instance, a Silver plan might still require a monthly premium of $200 and a deductible of $4,000—an insurmountable expense for families living paycheck to paycheck. This financial strain forces many to forgo coverage, opting instead to risk catastrophic health expenses.
The impact of income on insurance status also varies by state, particularly in those that have not expanded Medicaid under the ACA. In states like Texas and Florida, where Medicaid expansion was rejected, adults earning below 100% of the federal poverty level ($14,580 for an individual in 2023) fall into the "coverage gap"—they earn too much to qualify for traditional Medicaid but too little to afford subsidized marketplace plans. This policy-driven exclusion disproportionately affects low-income workers in industries like retail and food service, where employer-sponsored insurance is rarely offered.
To mitigate these disparities, targeted interventions are essential. For individuals earning below $30,000 annually, exploring Medicaid eligibility or ACA marketplace subsidies is critical. Practical steps include using the Healthcare.gov calculator to estimate costs and checking state-specific Medicaid rules. For those in the coverage gap, community health centers offer sliding-scale fee services, though these are not a substitute for comprehensive insurance. Employers can also play a role by advocating for Medicaid expansion in non-expansion states, which would extend coverage to millions of low-income workers.
Ultimately, the link between income and insurance status underscores a broader systemic issue: healthcare affordability remains out of reach for many Americans, particularly those with limited financial resources. Until policies address the root causes of cost barriers, income will continue to dictate access to care, perpetuating health inequities across socioeconomic lines.
Life Storage Insurance: Is It a Requirement?
You may want to see also
Explore related products



![]()
State-by-state uninsured population variations
The uninsured rate in the United States varies dramatically from state to state, influenced by factors like Medicaid expansion, income levels, and policy decisions. For instance, as of 2023, Texas has one of the highest uninsured rates at approximately 18%, largely due to its decision not to expand Medicaid under the Affordable Care Act. In contrast, states like Massachusetts, with its pioneering healthcare reform, boast an uninsured rate below 3%. This disparity highlights how state-level policies directly impact access to healthcare.
Analyzing these variations reveals a clear pattern: states that expanded Medicaid have significantly lower uninsured rates. For example, California, which embraced Medicaid expansion, has reduced its uninsured rate to around 7%. Meanwhile, states like Florida and Georgia, which have not expanded Medicaid, continue to struggle with uninsured rates above 12%. This suggests that federal policies alone are insufficient—state-level action is critical in closing coverage gaps.
To address these disparities, policymakers and advocates should focus on targeted strategies. States with high uninsured rates could consider Medicaid expansion, which has proven effective in reducing uninsured populations. Additionally, public awareness campaigns about available subsidies and enrollment periods can help individuals navigate the complexities of healthcare sign-ups. For example, during the 2023 open enrollment period, states like New York ran successful campaigns that increased sign-ups by 15%.
Comparatively, states with low uninsured rates offer valuable lessons. Massachusetts, for instance, combines Medicaid expansion with a state-run health insurance marketplace and an individual mandate, ensuring near-universal coverage. Other states could adopt similar models, tailored to their demographics and economic conditions. For example, a state with a large rural population might prioritize telehealth initiatives to improve access alongside policy changes.
In conclusion, state-by-state uninsured population variations are not inevitable but rather a reflection of policy choices and implementation strategies. By studying successful models and addressing barriers to coverage, states can significantly reduce their uninsured rates. Practical steps include expanding Medicaid, simplifying enrollment processes, and leveraging federal funding opportunities. The takeaway is clear: reducing uninsured rates requires both political will and targeted action at the state level.
Does Esure Offer Motorbike Insurance? A Comprehensive Coverage Guide
You may want to see also
Explore related products






![]()
Effects of policy changes on uninsured rates
Policy changes have a direct and measurable impact on uninsured rates in the United States, often serving as a lever to either expand or contract access to healthcare. For instance, the Affordable Care Act (ACA), implemented in 2010, led to a significant reduction in the uninsured rate by introducing Medicaid expansion, health insurance marketplaces, and subsidies for low-income individuals. Between 2010 and 2016, the uninsured rate dropped from 16% to 8.6%, demonstrating the power of policy to reshape healthcare access. However, subsequent policy shifts, such as the elimination of the individual mandate penalty in 2019, have contributed to a slight uptick in uninsured rates, highlighting the fragility of these gains.
Analyzing the effects of policy changes requires examining both federal and state-level actions. States that expanded Medicaid under the ACA saw larger reductions in uninsured rates compared to those that did not. For example, Kentucky’s uninsured rate fell from 14.3% in 2013 to 5.8% in 2016 after expanding Medicaid, while Texas, which opted out, saw a smaller decline from 22.1% to 16.6%. This disparity underscores the importance of state-level decisions in amplifying or mitigating federal policies. Policymakers must consider these variations when designing interventions to ensure equitable outcomes across regions.
A persuasive argument for policy-driven solutions lies in their ability to address systemic barriers to healthcare access. For instance, the Children’s Health Insurance Program (CHIP) has consistently maintained low uninsured rates among children by providing affordable coverage to families with incomes too high for Medicaid but too low for private insurance. Since its inception in 1997, CHIP has reduced the uninsured rate among children to less than 5%, serving as a model for targeted policy interventions. Expanding such programs to other vulnerable populations, such as low-income adults, could further reduce uninsured rates nationwide.
Comparatively, policy changes that restrict access to healthcare yield predictable increases in uninsured rates. For example, stricter eligibility requirements for Medicaid or reduced funding for outreach and enrollment assistance can deter eligible individuals from signing up. In 2018, states that implemented work requirements for Medicaid saw enrollment declines, even though many applicants met the criteria. This suggests that administrative barriers, rather than ineligibility, often drive disenrollment. Policymakers must weigh the unintended consequences of such measures, as they can exacerbate disparities in healthcare access.
To maximize the impact of policy changes, a multi-pronged approach is essential. First, expand Medicaid in all states to cover the remaining gaps in coverage, particularly in the South and Midwest. Second, restore and increase funding for outreach programs to educate eligible individuals about available options. Third, reintroduce incentives for purchasing health insurance, such as a reinstated individual mandate or enhanced subsidies. By combining these strategies, policymakers can create a more resilient healthcare system that withstands political fluctuations and ensures sustained reductions in uninsured rates.
Ensuring R Package Safety: Best Practices for Secure Installation
You may want to see also
Frequently asked questions
As of 2023, approximately 8-10% of Americans, or roughly 27-30 million people, do not have healthcare insurance, though numbers may vary based on the source and timing of data collection.
The main reasons include high insurance costs, lack of employer-sponsored coverage, ineligibility for public programs like Medicaid, and gaps in coverage options for certain income groups.
The number of uninsured Americans has fluctuated in recent years. While the Affordable Care Act (ACA) initially reduced uninsured rates, recent trends show slight increases due to factors like policy changes, economic shifts, and state-level variations in Medicaid expansion.
Low-income individuals, young adults, people of color, and those living in states that have not expanded Medicaid are disproportionately likely to be uninsured.