The question of how many Americans have health insurance is a critical issue that reflects the state of the nation’s healthcare system and its accessibility. As of recent data, the majority of Americans are covered by some form of health insurance, with employer-sponsored plans being the most common source. However, millions still remain uninsured, often due to factors such as cost, eligibility restrictions, or gaps in public programs like Medicaid and Medicare. Understanding these numbers is essential for policymakers, healthcare providers, and the public, as it highlights disparities in access to care and informs efforts to improve coverage and reduce barriers to health services.
Explore related products






What You'll Learn
- Employer-Sponsored Coverage: Majority of Americans get health insurance through their jobs or family members' employers
- Government Programs: Medicaid, Medicare, and CHIP provide coverage for low-income, elderly, and disabled individuals
- Individual Market: Some purchase private plans directly, often via Healthcare.gov or state marketplaces
- Uninsured Rates: Despite coverage gains, millions remain uninsured due to cost, eligibility, or choice
- Coverage Disparities: Insurance rates vary by age, income, race, ethnicity, and geographic location
![]()
Employer-Sponsored Coverage: Majority of Americans get health insurance through their jobs or family members' employers
Employer-sponsored health insurance is the cornerstone of the American healthcare system, covering approximately 155 million workers and their dependents, or about 56% of the insured population. This arrangement, where employers subsidize or fully cover premiums, has been a staple since World War II wage controls incentivized companies to offer benefits instead of higher salaries. Today, it remains the most common pathway to coverage, with 70% of private-sector employees having access to such plans, though uptake varies by company size—only 50% of small businesses (under 50 employees) offer this benefit compared to 96% of large firms.
Consider the mechanics: Employers negotiate group rates with insurers, often at lower costs than individual plans, and contribute an average of 82% toward employee-only coverage and 70% for family plans. Employees typically pay the remainder through payroll deductions, averaging $1,300 annually for individual coverage and $6,000 for families. This system ties healthcare to employment, creating both stability for insured workers and vulnerability for those in part-time, gig, or low-wage roles. For instance, a full-time retail worker at a major chain might receive comprehensive coverage, while their counterpart at a small boutique likely goes without.
The tax advantages further entrench this model. Employer contributions are exempt from income and payroll taxes, saving employees an estimated $300 billion annually. However, this exclusion disproportionately benefits higher earners, as the value of the tax break increases with income. A worker earning $50,000 saves roughly $1,500 in taxes through this exclusion, while someone earning $150,000 saves nearly $5,000—a regressive feature often criticized by policymakers.
Yet, this system is not without risks. Job loss can mean losing coverage, as seen during the 2008 recession when 10 million Americans lost employer-based insurance. COBRA allows continuation of coverage, but at full cost plus a 2% administrative fee, making it unaffordable for many. The Affordable Care Act (ACA) partially addressed this by expanding Medicaid and creating marketplaces, but employer-sponsored insurance remains dominant, leaving gaps for those ineligible for subsidies or Medicaid.
For individuals navigating this landscape, practical steps include evaluating job offers beyond salary to include health benefits, understanding open enrollment periods (typically November), and comparing employer plans to marketplace options during life changes like marriage or childbirth. Those in jobs without coverage should explore ACA subsidies, where 87% of enrollees pay less than $100/month after tax credits. While employer-sponsored insurance is a lifeline for millions, its limitations underscore the need for broader reforms to decouple healthcare from employment.
Unlocking Insurance Referrals: Proven Strategies to Secure Your Next Client
You may want to see also
Explore related products






![]()
Government Programs: Medicaid, Medicare, and CHIP provide coverage for low-income, elderly, and disabled individuals
In 2022, approximately 92% of Americans had health insurance, a figure that reflects the combined efforts of private insurers and government programs. Among these, Medicaid, Medicare, and the Children’s Health Insurance Program (CHIP) play a critical role in covering vulnerable populations. Together, these programs insure over 140 million Americans, including low-income families, seniors, and individuals with disabilities. Without them, the national uninsured rate would nearly double, underscoring their indispensable role in the healthcare system.
Medicaid, the largest of these programs, serves as a safety net for over 80 million low-income individuals and families. Eligibility varies by state but generally includes adults earning up to 138% of the federal poverty level (FPL), pregnant women, children, and individuals with disabilities. For example, a single adult in a state that expanded Medicaid under the Affordable Care Act (ACA) could qualify with an annual income of up to $18,754. Medicaid’s comprehensive benefits cover hospital stays, doctor visits, and long-term care, though specific services may differ by state. A key takeaway: if your income falls below your state’s threshold, Medicaid could provide immediate, affordable coverage.
Medicare, on the other hand, is designed for Americans aged 65 and older, as well as younger individuals with certain disabilities or end-stage renal disease. With over 65 million enrollees, it’s divided into parts: Part A (hospital insurance), Part B (medical insurance), and Part D (prescription drug coverage). While Part A is typically premium-free for those who paid Medicare taxes for at least 10 years, Part B requires a monthly premium, currently $174.70 in 2023. For low-income seniors, the Medicare Savings Programs can help cover these costs. Practical tip: enroll during your Initial Enrollment Period (the 7-month window around your 65th birthday) to avoid penalties.
CHIP fills a unique gap by covering children in families who earn too much for Medicaid but cannot afford private insurance. Serving nearly 10 million children, CHIP’s income limits vary by state but generally extend up to 200% of the FPL. For instance, a family of four could qualify with an annual income of up to $55,500 in some states. CHIP provides comprehensive benefits, including dental and vision care, often with no premiums or low copays. Parents should check their state’s CHIP website to determine eligibility and apply—a simple step that ensures children receive essential healthcare.
Collectively, these programs demonstrate a targeted approach to reducing health disparities. Medicaid’s expansion under the ACA, for example, has cut uninsured rates in participating states by nearly half. Medicare’s recent drug price negotiation powers, authorized by the Inflation Reduction Act, promise to lower out-of-pocket costs for seniors. Meanwhile, CHIP’s consistent funding ensures that children’s health remains a national priority. However, challenges persist, such as state-level variations in Medicaid eligibility and Medicare’s coverage gaps. For those navigating these programs, understanding eligibility criteria and available benefits is crucial—a small investment of time that can yield significant health and financial returns.
Strategies for Calling Life Insurance Leads
You may want to see also
Explore related products






![]()
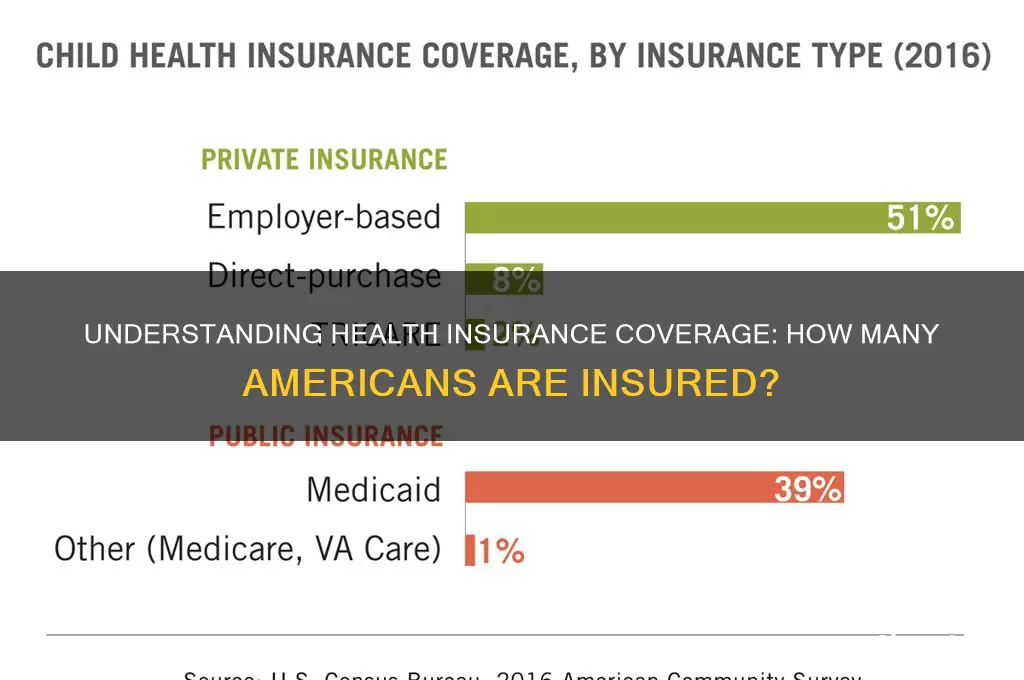
Individual Market: Some purchase private plans directly, often via Healthcare.gov or state marketplaces
In the individual health insurance market, millions of Americans bypass employer-sponsored plans and purchase coverage directly, often through platforms like Healthcare.gov or state-run marketplaces. This path offers flexibility but demands careful navigation. Unlike group plans, where employers subsidize premiums, individuals shoulder the full cost, making affordability a critical consideration. For instance, a 30-year-old nonsmoker in Texas might pay $300–$600 monthly for a mid-tier plan, depending on income and location. Subsidies, available to those earning up to 400% of the federal poverty level (e.g., $54,360 for an individual in 2023), can significantly reduce these costs. However, eligibility hinges on precise income calculations, requiring meticulous documentation during enrollment.
Navigating the individual market requires understanding plan tiers—Bronze, Silver, Gold, and Platinum—each with distinct cost-sharing structures. Silver plans, for example, often pair with cost-sharing reduction (CSR) subsidies for those earning up to 250% of the poverty level, lowering out-of-pocket expenses like deductibles and copays. A Silver plan might have a $3,000 deductible, but CSR could reduce it to $500 for eligible enrollees. Conversely, Bronze plans offer lower premiums but higher out-of-pocket costs, suitable for healthier individuals willing to risk higher expenses in exchange for monthly savings. Selecting the right tier involves balancing current health needs against financial stability.
Enrollment timing is non-negotiable in the individual market. Open Enrollment typically runs from November 1 to January 15, with coverage starting the following month. Missing this window confines individuals to Special Enrollment Periods (SEPs), triggered by life events like marriage, job loss, or relocation. For example, losing employer coverage grants a 60-day SEP to enroll in a marketplace plan without penalty. However, proving eligibility for an SEP requires documentation, such as a termination letter from an employer or a marriage certificate, adding complexity to an already stressful transition.
A common pitfall in the individual market is underestimating the importance of provider networks. Plans often restrict access to specific doctors or hospitals, particularly in HMOs (Health Maintenance Organizations). Before enrolling, individuals should verify that preferred providers are in-network to avoid unexpected out-of-network charges. For instance, a specialist visit might cost $200 in-network but soar to $600 out-of-network. Tools like Healthcare.gov’s provider search function allow users to cross-reference networks with their healthcare needs, ensuring continuity of care.
Finally, the individual market’s complexity underscores the value of professional guidance. Certified navigators or brokers, often available at no cost, can demystify plan details, estimate subsidy eligibility, and identify hidden costs. For example, a broker might highlight a plan’s limited prescription drug coverage, prompting a client to choose an alternative that better aligns with their medication needs. While DIY enrollment is possible, expert assistance can prevent costly mistakes and ensure optimal coverage. In a market where decisions carry significant financial and health implications, informed choices are not just beneficial—they’re essential.
Does CA Insurance Cover Windshield Repair or Replacement?
You may want to see also
Explore related products


![]()
Uninsured Rates: Despite coverage gains, millions remain uninsured due to cost, eligibility, or choice
Despite significant strides in expanding health insurance coverage, approximately 8% of Americans, or around 26 million people, remained uninsured in 2022. This figure, though lower than pre-Affordable Care Act (ACA) levels, highlights a persistent gap in access to healthcare. The reasons for this gap are multifaceted, rooted in financial barriers, eligibility restrictions, and personal choices. Understanding these factors is crucial for addressing the needs of the uninsured population and further reducing disparities in healthcare access.
Cost remains the most formidable barrier to health insurance coverage. Even with subsidies available through the ACA’s marketplaces, premiums, deductibles, and out-of-pocket costs can be prohibitively expensive for low-income individuals and families. For example, a Silver-level plan in 2023 had an average deductible of $4,800 for an individual, a sum that many cannot afford to pay upfront. Additionally, those who do not qualify for premium tax credits—often individuals earning just above the federal poverty level (FPL)—face the full brunt of these costs. Practical solutions include expanding Medicaid in the 10 states that have not yet done so, which would cover an estimated 2.2 million uninsured adults, and increasing subsidy eligibility to include those earning up to 200% of the FPL.
Eligibility restrictions further complicate access to coverage. Undocumented immigrants, for instance, are ineligible for Medicaid or ACA marketplace plans, leaving approximately 4.8 million people without a pathway to affordable insurance. Similarly, in states that have not expanded Medicaid, the "coverage gap" affects individuals earning too much to qualify for traditional Medicaid but too little to afford private insurance. This gap disproportionately impacts working-age adults in the South, where 9 of the 10 non-expansion states are located. Policymakers could address this by creating a federal fallback option for those in the coverage gap or extending Medicaid eligibility to all low-income adults regardless of immigration status.
Personal choice also plays a role in uninsured rates, though it is often intertwined with cost and awareness. Some individuals, particularly young and healthy adults, may forgo coverage because they perceive themselves as low risk for needing medical care. Others may be unaware of available options or struggle to navigate the enrollment process. For example, a 2021 survey found that 40% of uninsured adults did not know about ACA open enrollment periods. Community-based outreach programs, simplified enrollment processes, and targeted education campaigns could help bridge this knowledge gap. Additionally, offering catastrophic plans with lower premiums and higher deductibles might appeal to those who prioritize cost over comprehensive coverage.
Addressing uninsured rates requires a multi-pronged approach. While cost is the most significant barrier, eligibility restrictions and lack of awareness also contribute to the problem. Expanding Medicaid, increasing subsidies, and streamlining enrollment processes are actionable steps that could make a tangible difference. By tackling these issues, policymakers and healthcare advocates can move closer to the goal of universal coverage, ensuring that fewer Americans are left without access to essential healthcare services.
Selling Life Insurance: Can You Also Be a Licensed Adjuster?
You may want to see also
Explore related products
![]()
Coverage Disparities: Insurance rates vary by age, income, race, ethnicity, and geographic location
As of recent data, approximately 91% of Americans have health insurance, a significant improvement from past decades. However, this aggregate number masks deep-seated disparities in coverage that persist across demographic and geographic lines. Age, income, race, ethnicity, and location are critical factors that determine who remains uninsured or underinsured, revealing a fragmented healthcare landscape. Understanding these disparities is essential for addressing the root causes of inequity in access to care.
Consider age as a primary determinant of insurance status. While the Affordable Care Act (ACA) expanded coverage for young adults by allowing them to stay on parental plans until age 26, older adults, particularly those under 65, face higher premiums and limited options. For instance, a 60-year-old may pay up to three times more for insurance than a 21-year-old, even for the same plan. This pricing disparity, coupled with pre-existing conditions, leaves many in this age bracket vulnerable. Practical advice for this group includes exploring ACA subsidies, joining professional associations for group plans, or leveraging health savings accounts (HSAs) to offset costs.
Income inequality further exacerbates coverage gaps. Despite Medicaid expansion in many states, low-income individuals in non-expansion states often fall into the "coverage gap," earning too much for Medicaid but too little for ACA subsidies. For example, a single adult earning $12,000 annually in Texas—a non-expansion state—may not qualify for Medicaid but also find marketplace premiums unaffordable. To mitigate this, individuals should check eligibility for local safety-net programs or seek assistance from community health centers, which offer sliding-scale fees based on income.
Racial and ethnic disparities in insurance rates are equally stark. Data from the Kaiser Family Foundation shows that 7.8% of non-Hispanic Whites are uninsured compared to 19.1% of Native Americans and 18.3% of Hispanics. These disparities stem from systemic barriers, including language, immigration status, and occupational segregation into low-wage jobs without employer-sponsored insurance. Advocacy for culturally competent outreach programs and expanded Medicaid eligibility can help bridge these gaps. Employers can also play a role by offering multilingual enrollment assistance and ensuring benefits packages cater to diverse workforce needs.
Geographic location is another critical factor, with rural areas facing higher uninsured rates than urban centers. Rural residents often lack access to employer-sponsored insurance due to smaller job markets and face limited provider networks, making even insured care difficult to access. For example, in states like Mississippi and Texas, rural counties have uninsured rates exceeding 20%. Solutions include telemedicine expansion, mobile health clinics, and incentivizing healthcare providers to practice in underserved areas. Policymakers should prioritize funding for rural health infrastructure to address these disparities.
In conclusion, while overall insurance rates in the U.S. are high, coverage disparities persist along age, income, racial, ethnic, and geographic lines. Tailored solutions—such as age-specific financial tools, income-based safety nets, culturally sensitive outreach, and rural health initiatives—are necessary to ensure equitable access to care. Addressing these disparities requires a multifaceted approach, combining policy reform, community engagement, and innovative service delivery models.
Islamic Life Insurance: Halal Protection for Your Family
You may want to see also
Frequently asked questions
As of 2023, approximately 91% of Americans have health insurance, according to the Centers for Disease Control and Prevention (CDC).
About 9% of Americans, or roughly 30 million people, were uninsured as of 2023, based on CDC and Census Bureau data.
Elderly Americans aged 65 and older have the highest health insurance coverage rate, primarily due to Medicare, with nearly 100% coverage.
The ACA significantly reduced the uninsured rate, increasing coverage by expanding Medicaid, creating health insurance marketplaces, and allowing young adults to stay on parental plans until age 26.
Employer-sponsored health insurance is the primary source, covering about 54% of Americans, followed by Medicaid (19%) and Medicare (18%).