Every year, a staggering number of people worldwide succumb to preventable or treatable conditions due to lack of health insurance. This issue disproportionately affects low-income individuals and communities, where financial barriers often prevent access to essential medical care. Studies suggest that in countries without universal healthcare, uninsured individuals face higher mortality rates from conditions like heart disease, cancer, and diabetes, as delayed or forgone treatment exacerbates health outcomes. While exact figures vary by region, estimates indicate that tens of thousands of deaths annually could be averted with adequate insurance coverage, highlighting the urgent need for equitable healthcare policies.
| Characteristics | Values |
|---|---|
| Estimated Annual Deaths (US) | Approximately 30,000 (data varies, with estimates ranging from 18,000 to 45,000 depending on the study and methodology) |
| Primary Causes of Death | Preventable conditions like heart disease, cancer, diabetes, and infections due to delayed or forgone care |
| Demographics Most Affected | Low-income individuals, racial and ethnic minorities, and those in states without Medicaid expansion |
| Economic Impact | Higher healthcare costs overall due to untreated conditions worsening and requiring more expensive interventions |
| Policy Implications | Highlights the need for expanded healthcare access, such as Medicaid expansion and affordable insurance options |
| Data Source Reliability | Studies often rely on statistical modeling and assumptions, leading to varying estimates |
Explore related products






What You'll Learn
![]()
Global mortality rates linked to uninsured individuals
Lack of health insurance is a silent killer, contributing to millions of preventable deaths globally each year. Studies suggest that uninsured individuals face a 40% higher risk of mortality compared to those with coverage. This disparity stems from delayed or forgone medical care, often due to financial barriers. For instance, a 2017 study published in *The Lancet* estimated that 32,000 working-age Americans die annually due to lack of health insurance, primarily from treatable conditions like diabetes, hypertension, and infections. Globally, the World Health Organization (WHO) highlights that low-income countries, where insurance penetration is minimal, bear the brunt, with millions dying from preventable diseases like malaria, tuberculosis, and maternal complications.
Consider the lifecycle impact of being uninsured. Children without coverage are less likely to receive vaccinations, increasing their risk of infectious diseases. For adults, untreated chronic conditions like asthma or heart disease can escalate into life-threatening emergencies. Pregnant women without prenatal care face higher risks of complications, contributing to maternal mortality rates that are 50% higher in uninsured populations. Even in high-income countries, where healthcare infrastructure is robust, uninsured individuals often bypass preventive screenings, leading to late-stage diagnoses of cancers or other critical illnesses.
Addressing this crisis requires a multi-faceted approach. Governments can implement universal healthcare systems, as seen in countries like Germany and Canada, where mortality rates linked to lack of insurance are significantly lower. Subsidized insurance programs, such as India’s Ayushman Bharat scheme, target low-income populations, reducing out-of-pocket expenses that deter care-seeking. Employers can play a role by offering affordable health plans, while NGOs can bridge gaps through community health initiatives. For individuals, understanding local healthcare resources and advocating for policy changes can mitigate risks.
A comparative analysis reveals stark differences between insured and uninsured populations. In the U.S., uninsured adults are 25% more likely to die prematurely than their insured counterparts. Contrast this with the U.K., where the National Health Service (NHS) ensures universal coverage, resulting in lower mortality rates from preventable causes. Similarly, in sub-Saharan Africa, where insurance coverage hovers around 5%, preventable deaths account for over 60% of mortality, compared to less than 20% in regions with higher insurance penetration. These disparities underscore the urgent need for global health equity.
Finally, practical steps can reduce mortality linked to uninsured status. Individuals should explore government-funded programs, community health clinics, or charitable organizations offering free or low-cost care. Employers and policymakers must prioritize expanding coverage, particularly for vulnerable groups like gig workers and the elderly. Technological solutions, such as telemedicine, can improve access to care in underserved areas. By addressing financial barriers and increasing healthcare literacy, societies can significantly reduce the global toll of uninsured mortality.
Understanding Medical Insurance Claims: A Step-by-Step Guide
You may want to see also
Explore related products






![]()
Impact of insurance gaps on preventable deaths
Lack of health insurance doesn't just delay care; it can be a death sentence. Studies estimate that 29,000 to 45,000 Americans die annually due to lack of health coverage. These aren't inevitable tragedies; they're preventable deaths linked to a systemic failure to provide access to basic healthcare.
Consider the case of a 42-year-old uninsured man experiencing chest pain. Without insurance, he might delay seeking medical attention, fearing the cost. What could have been diagnosed as manageable angina through a timely EKG and medication becomes a fatal heart attack. This scenario isn't hypothetical; it's a recurring pattern. Uninsured individuals are 25% more likely to die prematurely than their insured counterparts, often from conditions like heart disease, cancer, and diabetes that are treatable with early intervention.
The impact of insurance gaps extends beyond individual tragedies. It creates a ripple effect, straining emergency departments as the last resort for care. Uninsured patients often present with advanced, costly-to-treat conditions, driving up healthcare costs for everyone. Closing these gaps isn't just a moral imperative; it's an economic necessity. Studies show that expanding Medicaid coverage, for example, leads to significant reductions in mortality rates among low-income adults, particularly from conditions like heart disease and cancer.
Think of insurance gaps as cracks in a dam. Left unrepaired, they widen, allowing a steady stream of preventable deaths. We have the tools to fix these cracks: expanding access to affordable coverage, investing in preventive care, and addressing the social determinants of health that contribute to disparities. The question isn't whether we can prevent these deaths; it's whether we have the will to do so.
Navigating Medical Insurance Between Jobs
You may want to see also
Explore related products






![]()
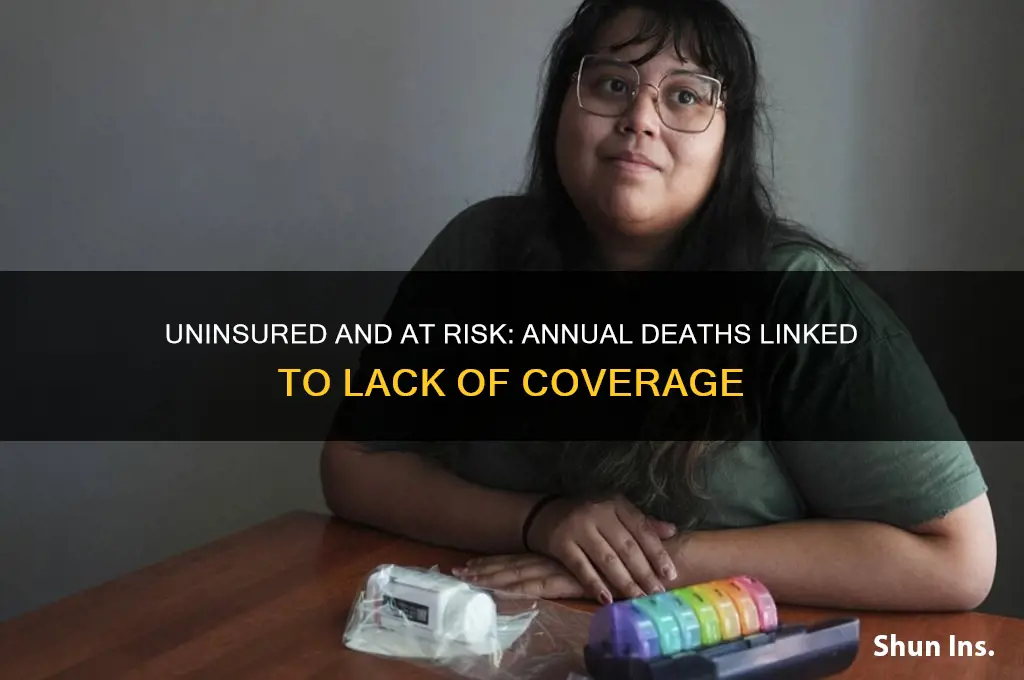
Regional disparities in uninsured death statistics
The impact of lacking health insurance on mortality rates is not uniformly distributed across regions, revealing stark disparities that demand attention. In the United States, for instance, studies indicate that uninsured individuals face a higher risk of premature death, with an estimated 30,000 to 45,000 excess deaths annually attributed to lack of coverage. However, these figures mask significant regional variations, influenced by factors such as state-level policies, socioeconomic conditions, and access to healthcare infrastructure.
Consider the contrast between states that expanded Medicaid under the Affordable Care Act (ACA) and those that did not. In expansion states, uninsured rates dropped dramatically, leading to a 6.1% reduction in mortality rates among low-income adults. For example, in Kentucky, a rural state with historically high uninsured rates, Medicaid expansion resulted in a 40% decrease in uninsured adults and a measurable decline in mortality. Conversely, non-expansion states like Texas and Florida continue to report higher uninsured rates and excess deaths, particularly among minority and low-income populations. This disparity highlights the critical role of policy decisions in shaping health outcomes.
Analyzing international data further underscores regional inequities. In countries with universal healthcare systems, such as Canada and the UK, deaths attributable to lack of insurance are virtually nonexistent. However, in nations with fragmented or privatized systems, regional disparities are pronounced. For instance, in India, urban areas with better access to private healthcare report lower uninsured death rates compared to rural regions, where public health infrastructure is often inadequate. This pattern illustrates how geographic and systemic factors intersect to create unequal health outcomes.
To address these disparities, policymakers must adopt targeted strategies. In the U.S., closing the Medicaid coverage gap in non-expansion states could save an estimated 7,000 to 17,000 lives annually. Similarly, in low- and middle-income countries, investing in rural health infrastructure and community-based insurance programs can mitigate regional inequities. Practical steps include leveraging data to identify high-risk regions, implementing culturally sensitive outreach programs, and fostering public-private partnerships to expand coverage.
Ultimately, regional disparities in uninsured death statistics are not inevitable but a reflection of policy choices and resource allocation. By focusing on evidence-based interventions and equitable distribution of healthcare resources, societies can reduce these disparities and ensure that geography does not dictate one’s chances of survival. The data is clear: lives are at stake, and the solutions are within reach.
Top RV Insurance Providers: Companies That Protect Your Mobile Home
You may want to see also
Explore related products

$8





![]()
Economic costs of uninsured-related fatalities
The economic toll of uninsured-related fatalities extends far beyond the human tragedy, embedding itself into the fabric of healthcare systems, labor markets, and societal productivity. Each year, an estimated 45,000 Americans die due to lack of health insurance, according to a 2009 study by Families USA. While this figure has been debated, the consensus remains: uninsured individuals face higher mortality rates due to delayed or forgone care. These deaths are not merely personal losses; they translate into quantifiable economic burdens. For instance, the average cost of a preventable hospitalization for an uninsured individual is approximately $15,000, compared to $10,000 for an insured patient, due to later-stage interventions. Multiply this by thousands of cases annually, and the financial strain on hospitals and taxpayers becomes staggering.
Consider the ripple effects on the workforce. Uninsured individuals who succumb to treatable conditions often belong to prime working-age groups (25–64). Their deaths result in lost productivity, estimated at $26 billion annually in the U.S. alone. Employers face higher turnover rates, recruitment costs, and reduced output, while families endure income loss and potential long-term poverty. For example, a 40-year-old uninsured breadwinner dying from untreated diabetes not only leaves a family without income but also removes a skilled worker from the labor pool, slowing economic growth. Policymakers must weigh these costs against the investment in preventive care and insurance coverage, which could mitigate such losses.
A comparative analysis reveals that countries with universal healthcare systems, such as Canada or the UK, spend less on uninsured-related fatalities. In the U.S., where 8.6% of the population remains uninsured (2022 data), the per capita healthcare cost is $12,914—nearly double that of Canada. This disparity underscores the inefficiency of a system where preventable deaths drive up expenses. Hospitals absorb $40 billion annually in uncompensated care for the uninsured, often shifting these costs to insured patients through higher premiums. This cycle perpetuates economic inequality, as lower-income individuals face both higher health risks and greater financial barriers to care.
To address these costs, actionable steps include expanding Medicaid coverage, subsidizing private insurance for low-income workers, and investing in community health programs. For instance, states that expanded Medicaid under the Affordable Care Act saw a 6.1% reduction in uninsured-related deaths within five years. Employers can also play a role by offering affordable health plans and wellness programs, reducing absenteeism and turnover. Individuals should prioritize preventive care, such as annual check-ups and screenings, which can detect conditions like hypertension or cancer early, saving up to $100,000 in treatment costs per case.
In conclusion, the economic costs of uninsured-related fatalities are not inevitable; they are a consequence of systemic gaps in healthcare access. By quantifying these losses—whether in hospital expenditures, workforce productivity, or societal well-being—we can build a compelling case for policy reforms and investments in universal coverage. The question is not whether we can afford to act, but whether we can afford the cost of inaction.
Key Questions to Ask About Accident Forgiveness
You may want to see also
Explore related products






![]()
Policy interventions to reduce uninsured deaths
Lack of health insurance is a silent killer, contributing to an estimated 30,000 deaths annually in the United States alone. This staggering number highlights a critical gap in healthcare access, one that policy interventions can and must address. By implementing targeted strategies, policymakers can significantly reduce uninsured deaths and ensure that healthcare becomes a right, not a privilege.
Expanding Medicaid eligibility is a proven, cost-effective solution. States that have expanded Medicaid under the Affordable Care Act have seen dramatic reductions in uninsured rates and improvements in health outcomes. For example, a 2020 study found that Medicaid expansion was associated with a 6.1% reduction in mortality rates among low-income adults. To maximize impact, policymakers should eliminate asset tests and streamline enrollment processes, ensuring that eligible individuals can access coverage without bureaucratic hurdles. Additionally, extending postpartum Medicaid coverage from 60 days to 12 months can address maternal mortality, a leading cause of uninsured deaths among women.
Subsidizing private insurance premiums can bridge the gap for those who fall above Medicaid eligibility thresholds but still struggle to afford coverage. The American Rescue Plan’s enhanced premium tax credits, for instance, reduced marketplace premiums by an average of $70 per person per month in 2021, leading to a record 14.5 million enrollments. Making these subsidies permanent and expanding eligibility to include more middle-income households could further reduce uninsured rates. Pairing subsidies with auto-enrollment options, where individuals are proactively enrolled in affordable plans unless they opt out, could increase uptake and save lives.
Investing in community health workers (CHWs) can address barriers to care beyond insurance status. CHWs serve as cultural brokers, helping uninsured individuals navigate the healthcare system, access preventive services, and manage chronic conditions. A study in Pennsylvania found that CHW interventions reduced hospital readmissions by 35% among low-income patients. Policymakers should allocate funding to train and integrate CHWs into primary care teams, particularly in underserved areas. Incentivizing CHW programs through Medicaid reimbursements could ensure sustainability and scalability.
Finally, addressing the root causes of uninsured deaths requires a comparative approach, learning from international models. Countries with universal healthcare systems, such as Canada and the UK, have significantly lower uninsured rates and better health outcomes. While a single-payer system may not be politically feasible in the U.S., incremental steps like creating a public option or lowering Medicare eligibility age to 55 could provide a safety net for millions. By studying and adapting successful international strategies, the U.S. can move closer to eliminating uninsured deaths.
In conclusion, reducing uninsured deaths is not just a moral imperative but a policy challenge with actionable solutions. By expanding Medicaid, subsidizing premiums, investing in community health workers, and learning from global models, policymakers can save lives and build a more equitable healthcare system. The cost of inaction is measured in human lives—a price no society can afford to pay.
Humana Medicare: Legit or a Scam?
You may want to see also
Frequently asked questions
Studies estimate that approximately 30,000 to 45,000 people die annually in the U.S. due to lack of health insurance, as reported by research from *The American Journal of Public Health* and other sources.
Deaths are often linked to delayed or forgone medical care, untreated chronic conditions (e.g., diabetes, heart disease), and inability to afford medications or preventive services.
Yes, studies show that insured individuals have lower mortality rates, as insurance improves access to timely care, preventive services, and treatment for serious conditions.
Yes, low-income individuals, racial and ethnic minorities, and those in states without Medicaid expansion are disproportionately affected by lack of insurance and related mortality.
The U.S. has significantly higher rates of uninsured-related deaths compared to other developed countries with universal healthcare systems, where access to care is more equitable.